Labs and Lytes 038
Author: Dr Jessica Yun
Reviewer: Dr Sarah Yong
An intubated and sedated 51-year-old man has increasing oxygen requirement and low-grade fevers.
Q1. What are the differentials?
The differential is very broad given the limited history provided. However, following exclusion of a displaced or obstructed endotracheal tube, important acute causes of hypoxaemia and fever include:
- Pneumonia (including COVID19)
- Atelectasis/ collapse
- Aspiration
- Pulmonary embolism
- Pulmonary contusion
It is worth considering these differentials even though they are not classically associated with a low grade fever, as they are common or important not to miss:
- Pneumothorax
- Pulmonary oedema
- Bronchospasm
Q2. A repeat chest X-ray has been obtained (top image) and compared to the previous (bottom image). Describe the key changes.
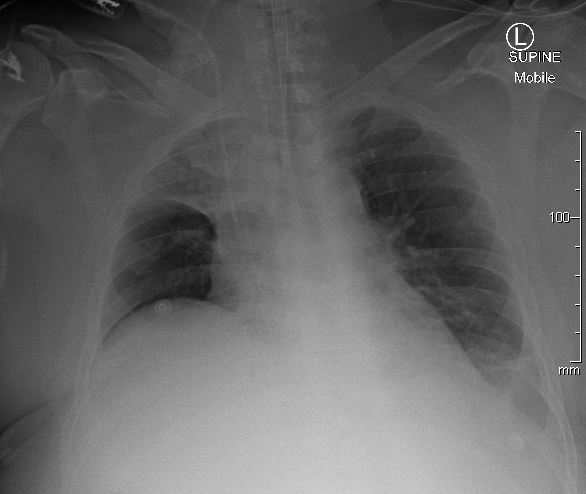
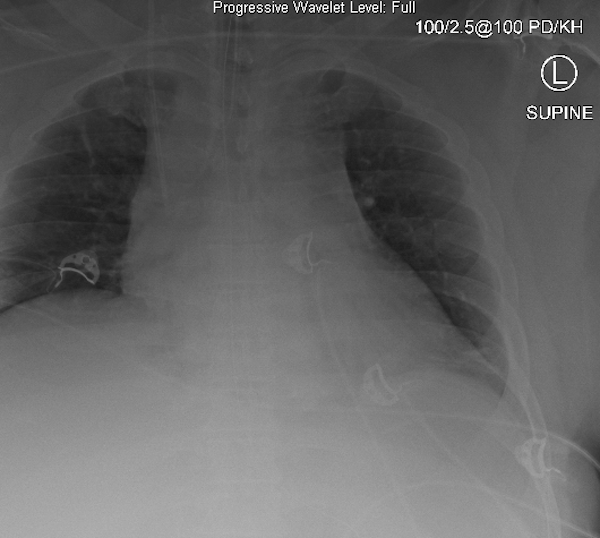
Figure 2. Previous CXR.
There is new development of the right upper lobe collapse.
- The left lower lobe collapse / effusion remains similar in appearance.
- Positions of ETT and right IJ CVC appears unchanged.
It is important to differentiate different causes of opacity from one another (e.g. collapse vs consolidation vs effusion).
Radiographic features of atelectasis include:
- Increased density opacity
- Crowding of pulmonary vessels
- Loss of volume +/- compensatory lung expansion of other lung regions
- Displacement of interlobar fissures, ipsilateral hemidiaphragm, and/or mediastinum toward the area of atelectasis
- Air bronchograms are not seen if there is central bronchial obstruction
Q3. What are the causes of atelectasis?
Causes of atelectasis can be classified into three anatomical categories:
- Intraluminal, for example:
- Mucous plugging which can be removed via bronchoscopy or chest physiotherapy
- Foreign bodies (e.g. aspirated blood clots or teeth in trauma)
- Endobronchial intubation which can be managed with correct placement of ETT and increasing PEEP
- Mural, for example:
- Tumour, e.g. malignancy
- Extramural, for example:
- extrinsic compression from surrounding anatomical structures (e.g. aneurysm, tumour)
Mucous plugging is common in intubated ICU patients.
Q4. What can be done to improve aeration of the collapsed lung segment(s)?
Intramural causes of atelectasis can be identified on bronchoscopy. Mucous plugs can be removed and bronchoalveolar lavage can be performed. Chest physiotherapy and trial of higher PEEP can be attempted in addition, or if bronchoscopy is unavailable.
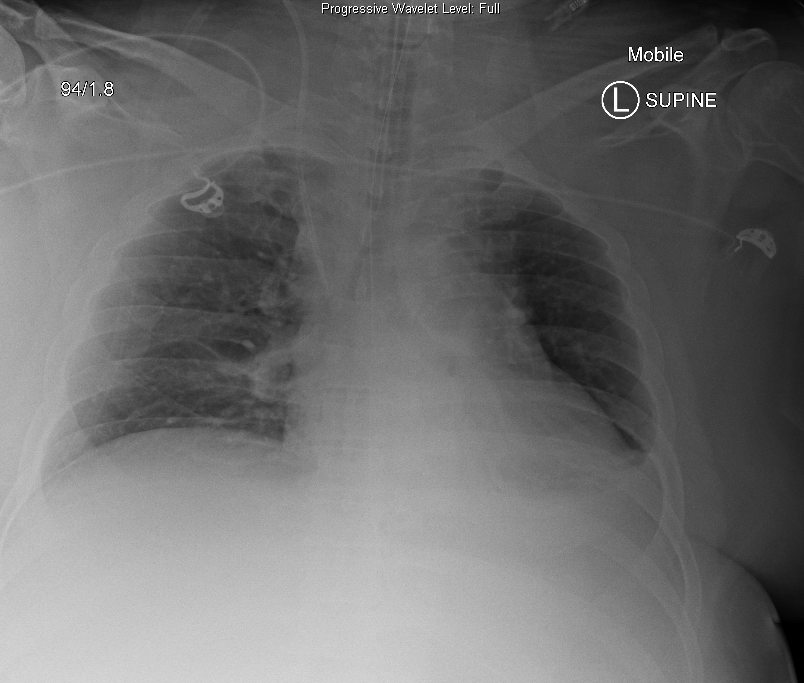
A thick sputum plug was removed from the right upper lobe via bronchoscopy. This is the chest X-ray post:
References
- Nickson CP. Atelectasis DDx. LITFL CCC. Accessed 29 July 2022. Available at URL: https://litfl.com/atelectasis-ddx/
- Young P. Collapse and Recruit. LITFL Clinical Cases. Accessed 29 July 2022. Available at URL: https://litfl.com/collapse-and-recruit/
- Nickson CP. Man versus Machine. LITFL Clinical Cases. Accessed 30 July 2022. Available at URL: https://litfl.com/man-versus-machine/
- Physiopedia. Respiratory Physiotherapy for ICU Patients. Accessed 29 July 2022. Available at URL: https://www.physio-pedia.com/Respiratory_Physiotherapy_for_ICU_Patients
All case-based scenarios on INTENSIVE are fictional. They may include realistic non-identifiable clinical data and are derived from learning points taken from clinical practice. Clinical details are not those of any particular person; they are created to add educational value to the scenarios.