Author: Dr Greg Brogan
Peer reviewer: Dr Matthew Durie, Dr Vinodh Nanjayya
Gautret P, Lagier JC, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial [published online ahead of print, 2020 Mar 20]. Int J Antimicrob Agents. 2020;105949. doi:10.1016/j.ijantimicag.2020.105949 [pubmed]
Introduction
Currently, there are growing numbers of COVID-19 cases and a lack of evidence of a disease- modifying treatment (Cortegiani, A. 2020, Frie, K. 2020, McIntosh, K. 2020). Hydroxychloroquine is a more soluble, less toxic form of Chloroquine with decades of safety data. It is used as an antimalarial and disease modifying agent in rheumatoid arthritis and systemic lupus erythematosus. There is recent evidence that it demonstrates in vitro activity against SARS-CoV-2 (Wang, M. 2020). At the time of this review, there is a scarcity of published data regarding the in vivo activity of hydroxychloroquine. This study (Gautret, P. 2020) details early results which have been released ahead of the yet to be published main paper.
Summary of Methodology
- This study is a non-randomised open label multicentre study conducted in the south of France in patients hospitalised with COVID 19
- It compares the effect of Hydroxychloroquine (200mg three times daily) both with and without azithromycin to a control group of no hydroxychloroquine.
- Inclusion criteria: Admitted to the Marseille centre, aged over 12 years of age and RT-PCR positive for SARS-CoV-2 in a naso-pharyngeal sample at admission
- Exclusion Criteria: Known contraindication to treatment (allergy, retinopathy, G6PD deficiency, QT Prolongation), pregnant or breastfeeding.
- The control group: Those who refused treatment, had an exclusion criteria, and patients presenting to other centres in Marseille and South France.
- The study was powered for 48 patients with an allowance for 10% loss to follow up.
- Primary endpoint was clearance of virus based on PCR at day 6 post inclusion
- Therapeutic drug monitoring for hydroxychloroquine was done using ultra-high performance liquid chromatography ultraviolet (UHPLC-UV) technology
Summary of Results
- 42 patients were enrolled of the targeted 48 and 6 were lost to follow up (16.7%) in the intervention arm leaving 36 patients for analysis.
- 20 patients received Hydroxychloroquine, 6 of which received azithromycin while 16 patients were in the control group.
- No statistically significant difference at baseline per se, however the intervention group trended to:
- be older (51.2 vs 37.3 years)
- Have a lower proportion of asymptomatic cases (10% vs 25%)
- Have a higher proportion of lower respiratory tract symptoms (30% vs 12%).
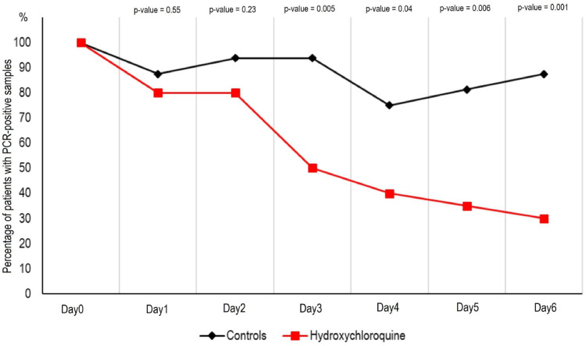
- On day 6, 70% of those treated tested negative vs 12.5% of the controls. This effect was seen as early as day 3 (50% negative vs 6.3% of the control group).
- Of those treated with hydroxychloroquine and azithromycin, 100% were negative at day 6 vs 57.1% with hydroxychloroquine alone vs 12.5% in the control group.
Study conclusions
- Hydroxychloroquine treatment was associated with a significant reduction in viral load
- This effect was reinforced by the use of azithromycin.
Study limitations
- This an ongoing trial
- It is underpowered
- The reported sample size does not reach the target (48) for its own power calculations
- It exceeds the predicted drop out rate of 10%
- All of those lost to follow up were in the treatment group with 3 being lost because of admission to Intensive Care and 1 because of death.
- There is no randomisation (risk of selection bias)
- Those excluded from the intervention were used as controls
- There is no use of placebo
- The study is unblinded (risk of performance bias)
- Some in the control group were managed in different centres to the intervention group
- The authors didn’t use appropriate statistical methods to account for repeated measurements in the same patient.
- The definition of a “negative” patient was based on one negative PCR result.
- It is evident that some control patients and one hydroxychloroquine + azithromycin patient became positive again after having a prior negative result.
- This paper reports only short term (up to 14 days) data, though there is still further findings to be published, medium and long term outcomes remain unknown.
Discussion
Since the publication of the Gautret paper, a couple of smaller studies have come to light, both finding no difference in the rate of virological clearance with combination hydroxychloroquine and azithromycin at 7 days (Molina, J. 2020, Chen, J. 2020). Additionally, the Chen study found no clinical or radiological difference in those treated and though the Gautret paper has not yet reported any adverse events, 1 patient in the Molina study was withdrawn because of prolonged QT interval. Currently, multiple further studies are underway (Clinicaltrials.gov 2020). This paper has many shortcomings and the reason for its current renown is more to do with the current void of evidence in this topic rather than any intrinsic value. It does not provide adequate evidence to support the use of hydroxychloroquine and more evidence is therefore required before we can consider hydroxychloroquine effective in the treatment of COVID-19.
References
- Chen, J., Danping, L., Ping, X et al. A pilot study of hydroxychloroquine in treatment of patients with common coronavirus disease-19 (COVID-19). J Zhejiang Univ. 2020, 49(1):0-0 DOI:10.3785/j.issn.1008-9292.2020.03.03 [No Pubmed Available]
- ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 4/4/2020. Cited 4/4/2020. Available from:https://clinicaltrials.gov/ct2/results?cond=COVID-19&term=Hydroxychloroquine&cntry=&state=&city=&dist= [No pubmed available]
- Cortegiani A, Ingoglia G, Ippolito M, Giarratano A, Einav S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19 [published online ahead of print, 2020 Mar 10]. J Crit Care. 2020;S0883-9441(20)30390-7. doi:10.1016/j.jcrc.2020.03.005 [pubmed]
- Frie, K, Gbinigie, K. Chloroquine and Hyrdorxychloroquine: Could these drugs be used to treat COVID-19. Oxford COVID-19 Evidence Service Team, Centre for Evidence Based Medicine, University of Oxford. (25.03.2020) https://www.cebm.net/covid-19/chloroquine-and-hydroxychloroquine-current-evidence-for-their-effectiveness-in-treating-covid-19/ Last accessed 4/4/2020 [No pubmed available]
- Gao J, Tian Z, Yang X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci Trends. 2020;14(1):72–73. doi:10.5582/bst.2020.01047 [pubmed]
- Gautret P, Lagier JC, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial [published online ahead of print, 2020 Mar 20]. Int J Antimicrob Agents. 2020;105949. doi:10.1016/j.ijantimicag.2020.105949 [pubmed]
- McIntosh, K. (2020) Coronavirus Disease 2019 (COVID-19) In: Hirsch, MS., BLoom, A. (Eds.) UpToDate. https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19?search=COVID%2019&source=search_result&selectedTitle=1~85&usage_type=default&display_rank=1#H1354847215 Last accessed 4/4/2020 [No Pubmed Available]
- Molina, J. M., Delaugerre, C., Le Goff, J., et al. No Evidence of Rapid Antiviral Clearance of Clinical Benefit with the Combination of Hydroxychloroquine and Azithromycin in Patients with Severe COVID-19 Infection. Med Mal. 2020. DOI:https://doi.org/doi:10.1016/j.medmal.2020.03.006 [No Pubmed Available]
- Wang M, Cao R, Zhang L, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020;30(3):269–271. doi:10.1038/s41422-020-0282-0 [pubmed]