Necessity is the mother of invention: COVID clinical subtypes in the absence of robust data
Author: Dr Aidan Burrell
Peer reviewers: Dr Lloyd Roberts, Dr Vinodh Nanjayya
Gattinoni L, Coppola S, Cressoni M, Busana M, Rossi S, Chiumello D. Covid-19 Does Not Lead to a “Typical” Acute Respiratory Distress Syndrome [published online ahead of print, 2020 Mar 30]. Am J Respir Crit Care Med. 2020;10.1164/rccm.202003-0817LE. doi:10.1164/rccm.202003-0817LE [pubmed]
Summary
Gattinoni and colleagues have published a fascinating editorial in Intensive Care Medicine which proposes a new clinical phenotype of patients presenting with COVID-19 viral pneumonia.
Patients with the new phenotype “Type L” present with profound hypoxaemia but have near normal pulmonary compliance. According to the editorial, this picture occurs in 50% of patients with COVID related pneumonia. This contrasts with the more “classic” model of ARDS where pulmonary compliance is more significantly reduced and total lung water is high (occurring in 20-30% of COVID-19 patients in their series).
This theoretical model was based on the “observation of 150 patients”, and “confirmed by colleagues in northern Italy”. No data or methods are provided in the editorial.
The phenotypes are:
Type L
- Low elastance (high compliance) with a low amount of non-aerated lung
- Low V/Q ratio, where hypoxaemia results from mismatched lung perfusion – due to a “loss of regulation of perfusion to the lung” and a “loss of hypoxic vasoconstriction”
- Low lung weight – Lung weight is only moderately high – as the infiltrates are only peripheral/subpleural
- Low lung recruitability – since the amount of non-aerated lung is low
- There is no respiratory distress as the lung compliance is ok
Type H
- High elastance (low compliance) from increased oedema
- High right-to-left shunt due to perfusion of poorly ventilated dependent/basal lung regions
- High lung weight due to increased lung water (approaching severe ARDS)
- High recruitability with a high amount of non-aerated lung which will recruit
The authors suggest these two phenotypes may be part of a spectrum of COVID disease, with the type L representing an earlier, less severe clinical state, progressing to a type H as worsening lung oedema, inflammation, patient – self inflicted lung injury (P-SILI) and iatrogenic damage lead to worsening lung injury and falling pulmonary compliance.
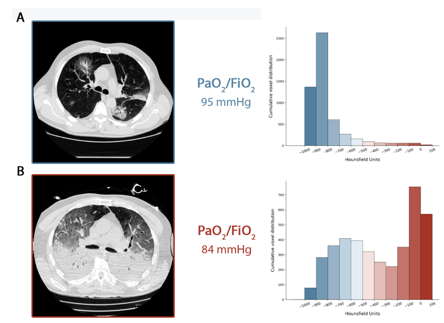
Figure 1. CT scans showing type L (A) and Type H (B) lung damage (Gattinoni et al, 2020). Source: 10.1164/rccm.202003-0817LE
The editorial recommends changes in management for the novel type L phenotype, including;
- Increase FiO2 to treat hypoxia (Type L will respond better, while type H will not)
- Type L trial of non invasive options including HFNP, and CPAP or NIV (though they note “non-invasive options are questionable”)
- Assess work of breathing (oesophageal manometry, swing of CVP or clinical detection)
- High PEEP may improve some patients by decreasing pleural pressure swings
- But high PEEP may worsen haemodynamics in patients with normal pulmonary compliance
- Intubate patients with high pleural pressure swings 15cmH2O
- Patients intubated with type L phenotypes can be ventilated at 8-9ml/kg (as the high compliance has less risk of VILI)
- Prone positioning should only be used as a rescue as the lungs are “too good”
Discussion
This model, produced by leaders in the field of Acute Respiratory Distress Syndrome (ARDS) and mechanical ventilation, articulates a novel way of thinking about pulmonary pathophysiology for COVID-19 pneumonia. Such theoretical models help us to (1) rapidly communicate new ideas about a disease, (2) may guide clinicians with their management choices, (3) provide a rationale for targeted interventions in future studies. The authors provide a logical pathophysiological argument for these phenotypes, and for new treatment strategies.
However, this hypothesis is based on small numbers of patients, primarily relying on anecdote and expert opinion. The small numbers of patients, and the lack of systematic analysis or scientific methodology, create a significant potential for bias, selectivity, and risk of over fitting of models. The lack of basic data presented about the patients, including demographics and treatments, means it is difficult to generalise to other populations. Furthermore, some of the treatment recommendations, such as recommending higher tidal volumes or avoiding prone positioning, while biologically plausible, are not based on high quality RCT data, and should be considered with extreme caution.
Conclusion
This editorial provides a logical and timely new model for understanding the different phenotypes of COVID 19 pneumonia. However clinicians should await further evidence that can investigate their clinical utility, and should be cautious when changing patient management based on these models.