Authors: Chris Nickson and Lloyd Roberts
Introduction
Tracheostomy patients are frequently seen in the ICU and at MET calls on the ward. The two major emergencies to be aware of (1) respiratory distress in a patient with a tracheostomy, and (2) haemorrhage from the tracheostomy site. In both situations, call for help early and seek senior assistance. Different tracheostomy tubes may have different features, the Portex® Blue Line Ultra® Tracheostomy Tube is most commonly used at the Alfred ICU (see Figure 1 below).
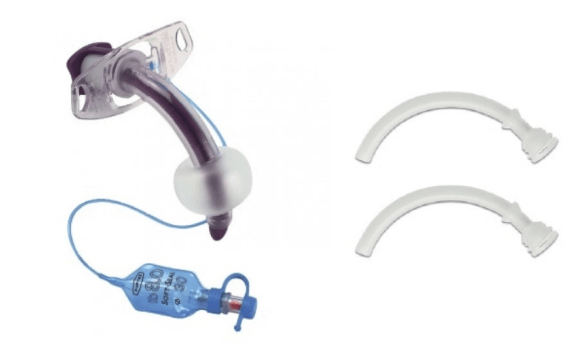
Figure 1. Portex® Blue Line Ultra® Tracheostomy Tube (left) and inner cannula (right). This device is always used with an inner cannula. Note that the size of a tracheostomy tube refers to the inner diameter, not the outer diameter. Tracheostomy tubes from different brands may have the same labelled size but differ in outer diameter, so they may not fit the same stoma. Images from Smith Medical.
Respiratory distress in a patient with a tracheostomy
Some key considerations in the management of respiratory distress in a patient with a tracheostomy:
- Call for help early and assess ABCs
- Provide high flow oxygen (e.g. FiO2 1.0) via the tracheostomy tube and face mask
- Deflate the tracheostomy cuff (if present), to allow oxygen to pass to the lungs from the mouth and nose.
- Confirm tracheostomy tube patency and position:
- Remove any speaking valves or caps.
- Remove inner cannula if present (it may be blocked).
- Pass a suction catheter and check for ETCO2 from the tracheostomy tube.
- The tracheostomy tube is blocked or displaced if:
- Suction catheter does not pass freely.
- No ETCO2 from the tracheostomy tube in a patient making spontaneous breathing attempts.
- If a tracheostomy is blocked or displaced, remove it and provide standard airway support (e.g. airway opening manoeuvres, airway adjuncts, FMV, SGA).
- If the tracheostomy tube patency and position are confirmed, consider other patient causes of respiratory distress and exclude equipment malfunction (e.g. disconnected oxygen supply).
Bleeding from a tracheostomy site
Bleeding from a tracheostomy site can be a life-threatening emergency. Early on, a small amount of bleeding (e.g. blood-stained sputum on suctioning) is common and is usually benign (e.g. due to the insertion procedure, suctioning, or manipulation of the tracheostomy tube). Late onset bleeding (>72h) is more concerning. It may be due to granuloma formation or infection but may also represent life-threatening erosion of an artery and/or formation of a tracheo-innominate fistula. These life-threatening conditions may initially present with a minor “sentinel” bleed followed by delayed life-threatening haemorrhage.
Some key considerations in the management of a bleeding tracheostomy site:
- Call for help early and assess ABCs.
- Clear the airway, e.g. blood clots may need to be suctioned, and bronchoscopy may be considered if sufficiently stable.
- Provide high flow oxygen (e.g. FiO2 1.0) via tracheostomy tube and facemask (if tracheostomy tube is cuff down or removed).
- Bleeding (especially if tracheo-innominate fistula is suspected) may be temporarily reduced or stopped by:
- applying finger pressure to the root of the neck in the sternal notch, or by
- optimising tracheostomy tube position and inflating the tracheostomy tube cuff (if present) with a 50ml syringe of air
- inflation should be done slowly and steadily to inflate the balloon to a maximum volume without bursting it
- usually, 10 to 35 mL is required in an adult depending on the type and size of the tracheostomy tube
- Correct coagulopathy and replace blood products as required.
- Ensure adequate IV access.
Tips and pitfalls
Some important tips and pitfalls to be aware of when managing a tracheostomy emergency:
- Get senior help ASAP.
- Do not provide positive pressure ventilation via a tracheostomy until patency and correct positioning have been confirmed. If the tube is displaced into the soft tissues of the neck, subcutaneous emphysema may occur leading to increased respiratory distress and making rescue attempts more difficult.
- Do not waste time attempting bronchoscopy down a tracheostomy tube in a severely hypoxic patient if the suction catheter does not pass freely and there is no ETCO2 detected – just remove the tracheostomy. In stable patients, senior clinicians may consider performing bronchoscopy to confirm tracheostomy patency and position.
- Check the indication for the tracheostomy tube – if laryngectomy or supraglottic pathology is present, intubation from above will not be possible.
- Check when the tracheostomy procedure was performed – it is only safe to reinsert tracheostomy tube if the tract is >7 days old.
References and further learning
These INTENSIVE posts concern issues with obstructed, displaced and bleeding trachestomies in a Q&A format:
References and useful resources:
- Alfred ICU Guideline – Tracheostomy Care (access for Alfred staff only)
- Alfred ICU flowchart – Alfred Health Tracheostomy Emergency Management (access for Alfred staff only)
Hess DR. Tracheostomy tubes and related appliances. Respir Care. 2005 Apr;50(4):497-510. Review. PubMed PMID: 15807912.[Free Full Text] - LITFL CCC — Bleeding tracheostomy
- LITFL CCC — Respiratory distress in a tracheostomy patient
- LITFL CCC — Tracheostomy tubes
- UK National Tracheostomy Safety Project, https://tracheostomy.org.uk/ (includes flowcharts)