Labs and Lytes 018
Author: Adam Drenzla
Reviewer: Diane Kelly
A young male was admitted to hospital with severe traumatic brain injury (TBI) following an assault. He was taken to theatre for emergent evacuation of his subdural haematoma (SDH) and placement of an external ventricular drain (EVD). On arrival to the ICU this was his chest radiograph (CXR):

Click to enlarge
Q1. Describe the abnormality on the CXR?
The left subclavian central venous catheter (CVC) tracks down the left mediastinal border instead of crossing the midline in the brachiocephalic vein and into the superior vena cava (SVC).
Q2. What is the differential diagnosis?
The CVC might be placed in an:
- Incorrect vascular structure: Descending aorta, Internal thoracic vein, Superior intercostal vein, Pericardiophrenic vein
- Anatomical vascular abnormality: Persistent left superior vena cava, Pulmonary vein via partial anomalous pulmonary venous drainage
- Extravascular structure: Pleura, Pericardium, Mediastinum
Q3. What simple bedside strategies can be employed to attempt to confirm position of the tip at the time of placement?
- Aspiration of blood: Inability to aspirate is consistent with, but does not confirm, extravascular placement
- Blood gas values: Can help distinguish between venous and arterial placement
- Transduction of the distal tip: Can confirm intravascular placement and differentiate between arterial and venous placement by allowing analysis of pressure waveforms.
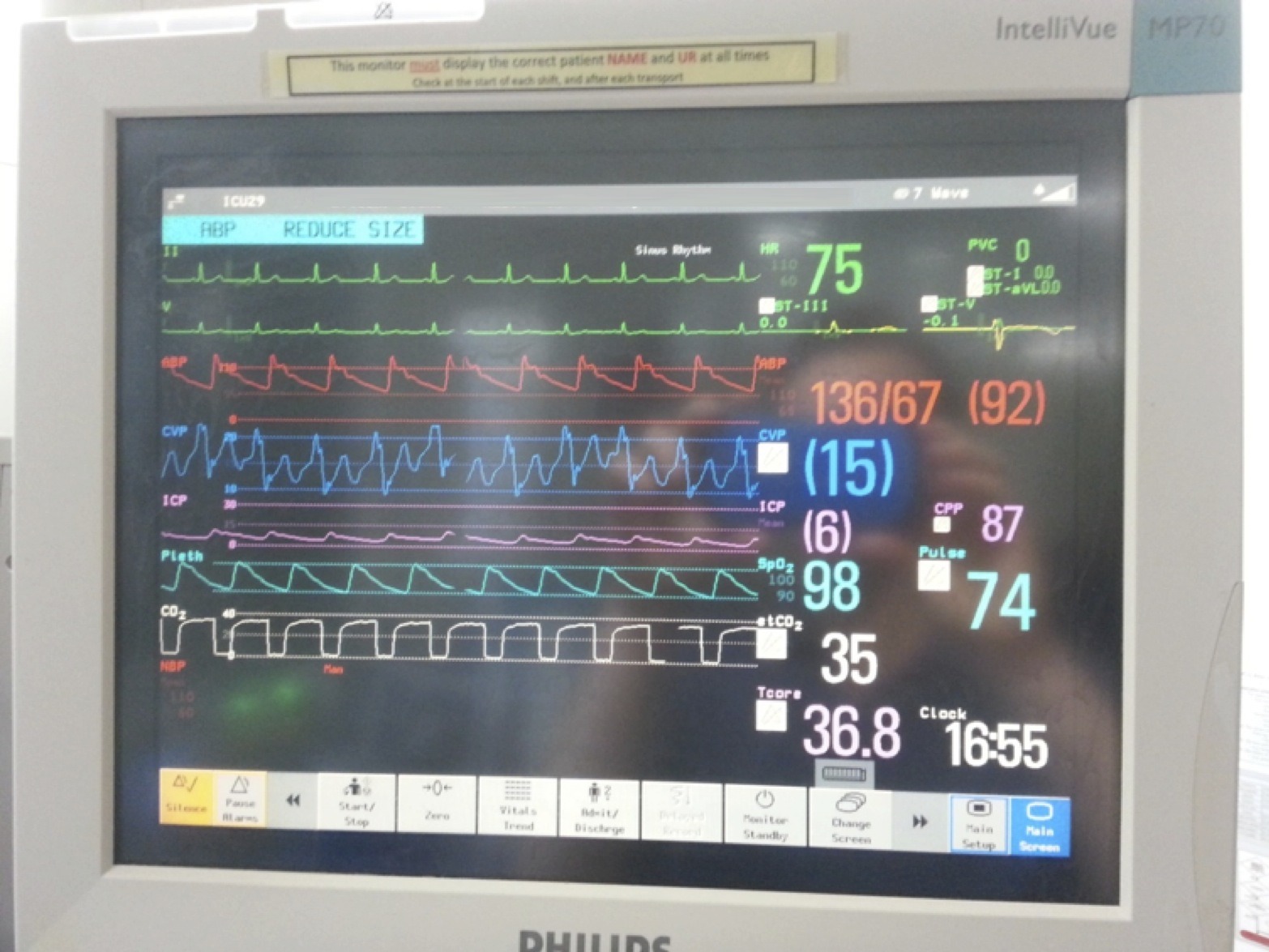
Q4. This was the monitor display when his lines were transduced. The blue line is the central line waveform. What does it show?
Click to enlarge
A central venous pressure (CVP) trace with a,c,v waves and x, y, descents
Q5. The blood gas drawn through the central line had an oxygen saturation of 92% while the blood gas drawn through the radial arterial line had an oxygen saturation of 97%. How might this be explained?
The tip location is likely to be a site where blood from the left and right-side of the heart is mixed.
It is unlikely this blood is from the right side of the circulation as the oxygen extraction would have to be severely reduced to explain such a high oxygen saturation. However it is clear the sample is not purely arterial given the lack of correlation with the radial artery sample.
Q6. What are the imaging options for definitive localisation?
- CT scan: This will help delineate the anatomy of the vessels and surrounding structures, however depending on the phase of the contrast study, it may not allow visualisation of the CVC tip.
- Bubble transthoracic echo (TTE) or transoesophageal echo (TOE): may identify the anatomical structure within which the tip lies, particularly if intravascular, and avoids exposure to radiation, but will not allow as accurate or easy anatomy delineation
- Contrast enhanced X-rays (so-called “linograms”): less radiation, but rarely performed
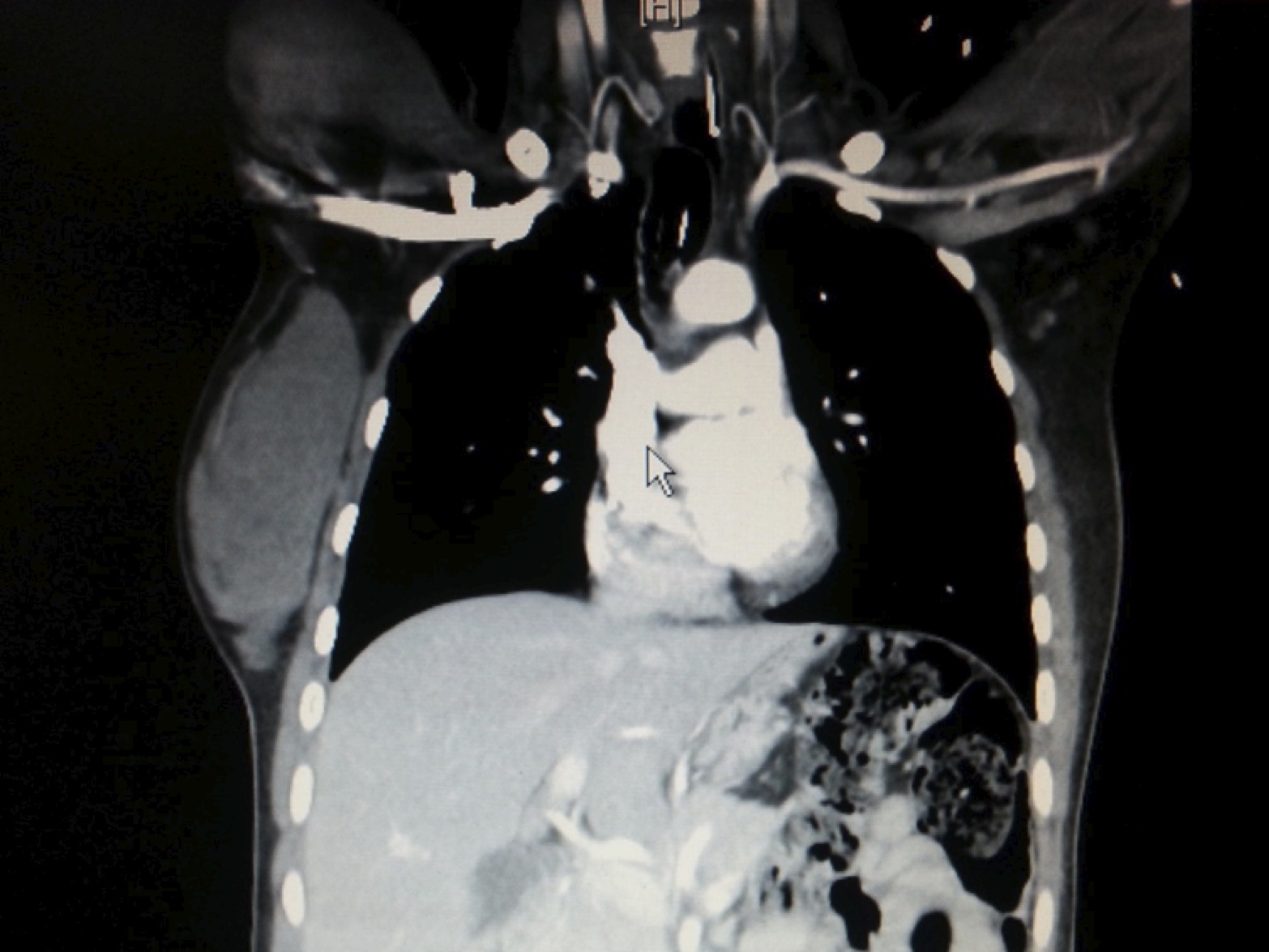
Q7. A CT was performed as part of the initial trauma admission prior to the central line being placed. These are three of the coronal sections. With regards to the central line, what do they show and where is the central line tip likely located?

Click to enlarge

Click to enlarge
Click to enlarge
There is a persistent left superior vena cava (PLSVC) which drains into the left atrium. There is no brachiocephalic vein.
The CVC tip is likely located somewhere near the junction of the SVC and left atrium. At this site there will be mixing of blood from the lungs and the systemic circulation that will account for the measured oxygen saturation.
Q8. List three facts about this finding?
Persistent left superior vena cava:
- Is the most common thoracic venous anomaly (0.5% of general population)
- Most commonly drains via the coronary sinus into the right atrium (it drains into the left atrium only 5-10% of the time)
- In up to 40% of cases there are other associated cardiac anomalies
Q9. What are the risks of central venous catheterisation in the context of this finding?
Risks of CVC insertsion into a persistent left superior vena cava include:
- increased mechanical complications on insertion
- risk of arrhythmias with wires in the coronary sinus
- if the tip is in a low flow system, such as the coronary sinus, infusions which require a high flow system should be avoided (for instance, hyperosmotic solutions such as TPN)
- when the PLSVC drains into the left atrium there is a risk of systemic embolization of air or particulate matter
Nevertheless, successful placement of pacing wires and swan ganz catheters into PLSVC draining into the right atrium are well described.
References and Links
- Biffi M, Bertini M, Ziacchi M, Martignani C, Valzania C, Diemberger I, Branzi A, Boriani G. Clinical implications of left superior vena cava persistence incandidates for pacemaker or cardioverter-defibrillator implantation. HeartVessels. 2009 Mar;24(2):142-6. doi: 10.1007/s00380-008-1091-4. Epub 2009 Apr 1.PubMed PMID: 19337799.
- Fares WH, Birchard KR, Yankaskas JR. Persistent Left Superior Vena Cava Identified During Central Line Placement: A Case Report. Respir Med CME. 2011;4(3):141-143. PubMed PMID: 22121390; PubMed Central PMCID: PMC3222566.
- Ghadiali N, Teo LM, Sheah K. Bedside confirmation of a persistent leftsuperior vena cava based on aberrantly positioned central venous catheter onchest radiograph. Br J Anaesth. 2006 Jan;96(1):53-6. Epub 2005 Nov 25. PubMed PMID: 16311276.
- Gibson F, Bodenham A. Misplaced central venous catheters: applied anatomy and practical management. Br J Anaesth. 2013 Mar;110(3):333-46. doi: 10.1093/bja/aes497. Epub 2013 Feb 5. Review. PubMed PMID: 23384735
- Goyal SK, Punnam SR, Verma G, Ruberg FL. Persistent left superior vena cava: acase report and review of literature. Cardiovasc Ultrasound. 2008 Oct 10;6:50.doi: 10.1186/1476-7120-6-50. Review. PubMed PMID: 18847480; PubMed Central PMCID:PMC2576163
- Pahwa R, Kumar A. Persistent left superior vena cava: an intensivist’sexperience and review of the literature. South Med J. 2003 May;96(5):528-9.Review. PubMed PMID: 12911199
- Povoski SP, Khabiri H. Persistent left superior vena cava: review of theliterature, clinical implications, and relevance of alterations in thoraciccentral venous anatomy as pertaining to the general principles of central venous access device placement and venography in cancer patients. World J Surg Oncol.2011 Dec 28;9:173. doi: 10.1186/1477-7819-9-173. Review. PubMed PMID: 22204758;PubMed Central PMCID: PMC3266648.
- Schummer W, Schummer C, Hoffmann E, Gerold M. Persistent left superior venacava: clinical implications for central venous cannulation. Nutr Clin Pract. 2002Oct;17(5):304-8. PubMed PMID: 16215005.