Labs and Lytes 006
Author: Nick Bingham
Reviewer: Chris Nickson
A 50 year-old man presented to the emergency department with jaundice and confusion.
These are his LFTs:
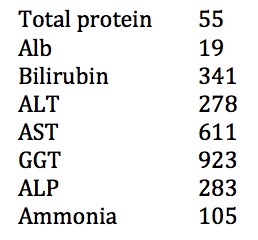
Q1. What diagnosis is this LFT pattern typical of?
The liver function tests are typical of acute alcoholic hepatitis.
- Typically an AST:ALT ratio of >2:1
- Modest rises in aminotransferases (rarely >500)
- Hyperbilirubinaemia
- Elevated GGT
- Elevated INR and hypoalbuminaemia (decreased liver synthetic function)
The approach to deranged liver function tests is to first recognise the pattern of derangement. This can be hepatocellular, cholestatic, a mixture of both, or an isolated hyperbilirubinaemia. The pattern is determined by looking at the AST, ALT and ALP. If ALT and AST are elevated out of proportion with the ALP, this is a hepatocellular pattern (e.g. hepatitis). If ALP is proportionately higher than ALT and AST, this is typical of a cholestatic picture.
Different aetiologies are associated with the different patterns. Our patient presented with a hepatocellular pattern of derangement.
A few notes on hepatitic pattern LFT derangement:
AST:ALT ratio of greater 2:1 is highly suggestive of alcoholic hepatitis
- Especially in the setting of GGT elevation
AST and ALT >1000 occurs in three main settings that are often easily differentiated
- Viral hepatitis — Clues in history, viral hepatitis serology
- Ischaemic hepatitis — Measure LDH (also elevated in paracetamol toxicity); note that the t1/2 of ALT is approximately one day. Therefore once the cause of ischaemia (hypotension) is corrected, the ALT should fall rapidly over the coming days.
- Paracetamol toxicity — History, paracetamol levels; remember to treat with N-acetylcysteine!
The patient has an mildly tender, easily palpable, firm, smooth-edged liver on examination of the right upper quadrant.
Q2. What does this suggest and what is the likely pathogenesis?
Hepatomegaly from alcoholic
Alcoholic hepatitis is associated with hepatocellular damage due to alcohol. In terms of pathophysiology this leads to hepatocyte “ballooning”, where the cells become highly swollen. In association with the fatty infiltration that is common with alcoholic liver disease, this can lead to hepatomegaly.
Hopefully a CT scan is not needed to diagnose such a large liver – palpation of the abdomen is a good place to start!
Q3. How useful is testing the ammonia level? What are the limitations?
Determining the ammonia level has many limitations
- Not required for diagnosis fo hepatic encephalopathy
- Levels are not consistently elevated
- Once >2x the upper limit of normal there is no longer a relationship with severity
- There are non-hepatic causes of ammonia increases, such as: renal disease, drugs, chemotherapy, TPN, porto-systemic shunting
- The level is affected by blood taking technique, and the sample must be transported on ice
Q4. Outline the specific management of this condition?
Determine if the patient should be treated with prednisolone
Calculate the Maddrey Score at day 0 (click here for the calculator on MDCalc)
- Determines severity of the alcoholic hepatitis and whether prednisolone may be of benefit
- Uses the bilirubin and prothrombin time
- If >32, prednisolone is given for 28 days
Calculate the Lille score at day 7 (click here for the LilleModel.com calculator)
- Determines whether the steroids have had an effect that justifies continuing them for the full 28 days
- Uses the change in bilirubin from D0 to D7, as well as the creatinine, albumin and prothrombin time at D0
- If score is >0.45 then it suggests that prednisolone has not been helpful – it may be worth stopping
- If >0.45 mortality approaches 75% at 6 months
General management
- Alcohol abstinence
- Hydration and nutritional support
- Infection surveillance
- GI protection
- appropriate supportive care and monitoring
Pentoxifylline
- Inhibits tumour necrosis factor synthesis (increased in alcoholic hepatitis patients)
- 400mg TDS is the usual dose
- Evidence is not as strong as for prednisolone
- Used in patients when prednisolone is contraindicated
- Not additive to steroids; so if the patient fails steroids there is no benefit to trialling or adding pentoxifylline
Seek and treat complications of alcoholic liver disease such as:
- ascites
- spontaneous bacterial peritonitis
- esophageal variceal bleeding
- hepatic encephalopathy
- hepatorenal syndrome
- hepatopulmonary syndrome
- portopulmonary hypertension
- hepatoma
Q5. What is the prognosis for this condition?
Prognosis largely depends on whether the patient remains abstinent from alcohol
5 yr survival after treatment of the acute episode
- 75% if abstinent
- 21% if continued drinking
- 27% if they relapse after stopping
References and Links
- Abenavoli L, Milic N, Rouabhia S, Addolorato G. Pharmacotherapy of acute alcoholic hepatitis in clinical practice. World J Gastroenterol. 2014 Mar 7;20(9):2159-67. doi: 10.3748/wjg.v20.i9.2159. Review. PubMed PMID: 24605014; PubMed Central PMCID: PMC3942820.
- Lucey MR, Mathurin P, Morgan TR. Alcoholic hepatitis. N Engl J Med. 2009 Jun 25;360(26):2758-69. doi: 10.1056/NEJMra0805786. Review. PubMed PMID: 19553649.
- Jaurigue MM, Cappell MS. Therapy for alcoholic liver disease. World J Gastroenterol. 2014 Mar 7;20(9):2143-58. doi: 10.3748/wjg.v20.i9.2143. Review. PubMed PMID: 24605013; PubMed Central PMCID: PMC3942819.
All case-based scenarios on INTENSIVE are fictional. They may include realistic non-identifiable clinical data and are derived from learning points taken from clinical practice. Clinical details are not those of any particular person; they are created to add educational value to the scenarios.