Author: Chris Nickson
Peer reviewers: Josh Ihle, Aidan Burrell, Arne Diehl
Everything ECMO 018
A 60-year-old woman was retrieved from a regional hospital on VA ECMO. The cannulae were inserted using a surgical ‘cut down’ technique, rather than a percutaneous Seldinger technique. She is having ongoing bleeding from the return site (arterial) in her right groin.
An additional suture is inserted to try to create a ‘purse string’ around the cannula insertion site. Suddenly there is profuse bleeding at the site and an emergency call is activated.
Q1. What has happened?
Profuse bleeding in this setting is due to circuit rupture at the cannula insertion site until proven otherwise. Other possibilities are a disconnection at a junction, inadvertent removal or withdrawal of an ECMO cannula or accidental arterial puncture with the suture needle.
ECMO cannulae are prone to devastating rupture if punctured by a needle. The flat metal wire reinforcing the cannula is held together on the outside by half a millimetre thick polyurethane plastic. Once the plastic is breached, the metal wire unravels and loses its structure. If this happens to the return cannula, it tends to rupture suddenly with rapid blood loss as the post-pump region of the circuit returning blood to the aorta is under positive pressure. The patient is at risk of extremely rapid exsanguination.
Deirdre Murphy talks about this complication of suturing in ECMO cannulae, and how it led to a change in practice at the Alfred ICU, in her smaccGOLD talk ECMO: What could go wrong?
Q2. What should be your immediate actions?
The approach to post-pump-head circuit rupture is as described in Everything ECMO 017.
- Immediately clamp the circuit proximal and distal to the rupture site and turn off pump.
- Call for help and contact the ICU Consultant and ECLS Coordinator
- Support patient circulation (ALS measures) if required
- Recannulation is required as the return cannula has been breached (see below)
- Restart ECMO once the return cannula is replaced and all clamps are removed
Options for recannulation are complex and there are multiple options:
- Clamp the return cannula closer to the skin beyond the breach. In this situation this is likely below skin level and would involve withdrawing the cannula with risk of even more bleeding. Clamping the metal wire component also precludes re-wiring.
- Attempt to rewire the cannula, which has to be done swiftly given the inability to compress the site whilst feeding the wire. The wire can potentially be caught in the structural damage of the cannula.
- Remove the entire return cannula and cannulate alternate site. This requires a dedicated person for compression of the large defect in the vessel and requires subsequent surgical support.
- Clamp return cannula, compress site of damage and recannulate alternate site. The point for compression maybe poorly identifiable proximal to the entry at the skin. This option will also require surgical removal of the cannula.
Needless to say, this is a very bad situation indeed! The risk of mortality is high, as the patient will likely need cardiopulmonary resuscitation with chest compressions if VA ECMO dependent, which may be compounded by severe haemorrhage, until the return cannula can be replaced. Should the patient survive he or she will be at risk of line sepsis as sterility is likely compromised in any of the above recannulation options.
ECMO cannulation is discussed in Everything ECMO 010.
Q3. How can bleeding from a cannulation site be prevented?
In short:
- Avoid cut-downs
- Correct underlying bleeding diatheses
Apart from strictly monitoring APTT (or Anti-Xa) levels in heparinised patients, and correcting any underlying bleeding diathesis appropriately, the main measure used at the Alfred ICU to prevent bleeding from the ECMO cannula sites is to avoid any ‘cut downs’ during cannula insertion. An ultrasound-guided, percutaneous technique of cannula insertion is used:
- Seldinger technique is used (i.e. needle puncture, insert guidewire, perform sequential dilatation over the guidewire, then insert the cannula over the guidewire)
- Serial dilation avoids the need for any skin incision in the majority of cases, and ensures there is a tight skin seal around the cannula preventing bleeding. Occasionally during especially difficult dilation, a small – no more than 50% of the diameter of the cannula – incision is made (using the “scalpel of shame”).
- For effective sequential dilatation, the dilator is advanced carefully along the course of the guidewire. Once tissue resistance is met the dilator should be ‘rolled’ or rotated to put further tension on the connective tissues resisting the advancement of the dilator. The dilator is removed with the torque still applied (i.e. “go in straight, come out twisted”… just like Medical School as Vin Pellegrino says). This action breaks down the connective tissues and allows further advancement of the dilator on reinsertion.
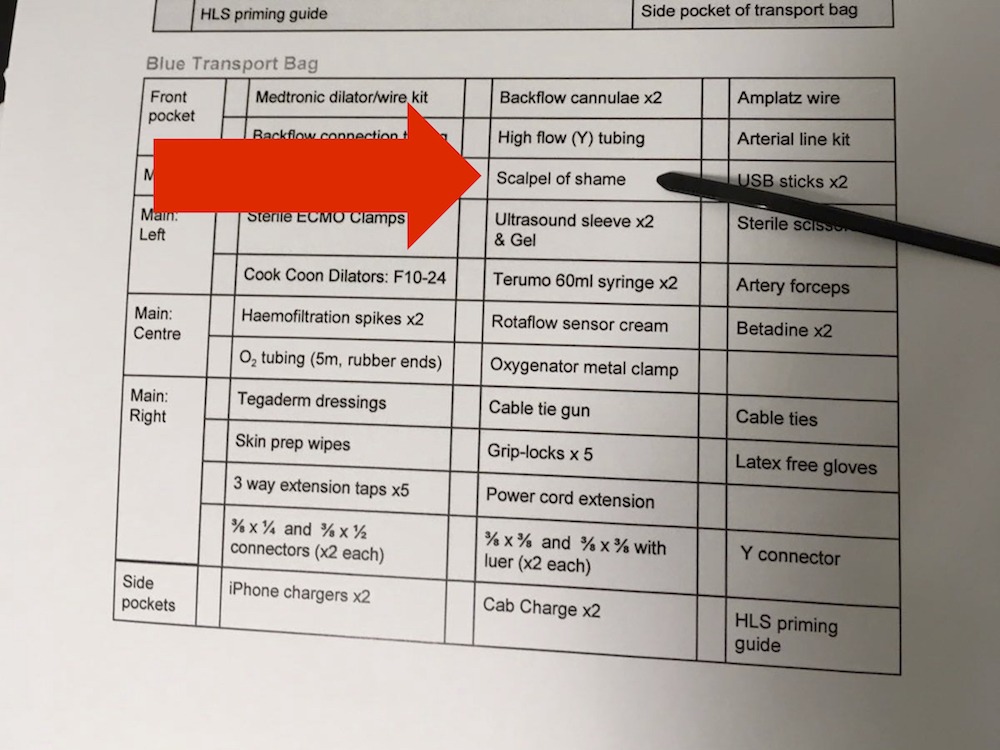
Alfred ICU ECMO Transport Checklist – don’t forget the “scalpel of shame”!
Q4. How are ECMO cannula secured without using sutures?
The steps involved are:
- Clean and dry the skin around the cannula insertion site
- Cover and secure the cannula with a sterile transparent dressing, which overlies the insertion site
- Fix the cannula tubing to the patient’s body (e.g. the leg) at two sites using adhesive Velcro supports (Lovell skin tabs, often called by the manufacture name ‘GRIP-LOK’)
- Apply the proximal GRIP-LOK close to the skin insertion site of cannula to reduce the potential length of unsecured line, which can be caught and pulled upon, moving the cannulae or even causing a decannulation.
Securing ECMO cannulae in this fashion removes the need for the use of sutures to secure the ECMO cannula. This negates the risk of a suture needle puncturing the ECMO cannula or causing more bleeding from the suture sites.

Grip-LOK securement of an arterial ECMO cannula.
Reference
- Pellegrino V, Sheldrake J, Murphy D, Hockings L, Roberts L. Extracorporeal Membrane Oxygenation (ECMO). Alfred ICU Guideline, 2012.