As prepared by Chris Nickson, here are the practice written questions from a recent CICM Second Part exam practice session at The Alfred ICU, with recommended reading from LITFL.com Critical Care Compendium and other FOAM sources:
Q1.
Discuss vasoplegia in ICU patients, including the underlying mechanisms and consideration of treatment options. (100%)
Learn more here:
- Lambden, S., Creagh-Brown, B.C., Hunt, J. et al. Definitions and pathophysiology of vasoplegic shock. Crit Care 22, 174 (2018). https://doi.org/10.1186/s13054-018-2102-1
- Levy, B., Fritz, C., Tahon, E. et al. Vasoplegia treatments: the past, the present, and the future. Crit Care 22, 52 (2018). https://doi.org/10.1186/s13054-018-1967-3
Possible approach to answering this very big question:
VASOPLEGIA
OVERVIEW
- No consensus definition
- Characterised by
- Decreased SVR
- due to arteriolar dilatation
- due to decreased vascular smooth muscle (VSM) constriction
- normal or hyperdynamic cardiac function (however cardiac dysfunction can co-exist with vasoplegia)
- May or may not involve vasoplegic shock (distributive shock), characterised by hyperfusion (high lactate carries worse prognosis)
- Often associated with relative hypovolaemia from increased venous capacitance and capillary leak
- Has multifactorial causes, is common in ICU, and is associated with morbidity and mortality
MECHANISMS
- Contractile state of VSM is primarily determined by intracellular calcium, which is affected by ATP-sensitive K channels that determine depolarisation state
- Factors affecting vascular smooth muscle contractility are:
- EXTRINSIC
- Sympathetic nervous system
- Endocrine
- Glucocorticoids
- Catecholamines
- Thyroid hormones
- Vasopressin
- INTRINSIC
- Endothelial secretions
- NO
- PGI2
- ET1
- Metabolites
- Acidemia
- Hypoxia
- ROS
- Autacoids
- 5HT
- Prostaglandins
- TXA2
- Endothelial secretions
- EXTRINSIC
- These processes are dysregulated in pathological states by cytokine cascades triggered by DAMPS (damage-associated molecular patterns, e.g. HSPs, nucleic acids) and PAMPS (pathogen-associated molecular patters, e.g. LPS) that bind PRR (pattern recognition receptors, e.g. Toll-like receptors), as well as other mechanisms PAMPS – sepsis
- PAMPS and DAMPS – post-op, post-bypass, post-arrest, transfusion, pancreatitis
- DAMPS – burns, trauma, any other cause of shock
- Other – GA, epidural, neurogenic, anaphylaxis, vasodilatory drugs and toxins
TREATMENT
- Seek and treat underlying cause
- E.g. antibiotics for infection, stop vasodilatory drugs
- Determine appropriate MAP target
- E.g. >65 mmHg for septic shock (SSC guidelines) and most patients
- Can individualise to patient (but evidence lacking)
- E.g. tolerate MAP >60 if no shock, otherwise well and likely short-lived cause to prevent SEs/ complications of vasopressors
- E.g. higher DBP target if known CAD to ensure coronary perfusion
- E.g. MAP 80 may be preferred in neurogenic shock from spinal cord injury
- Correct hypovolaemia and metabolic state
- E.g. up to 30 mL/kg IBW for septic shock
- Consider HCO3/ RRT for severe acidemia (controversial, unclear thresholds)
- O2 therapy to targt SpO2 92-96% in most patients
- Thiamine if suspected deficiency or hyperlactemia
- Calcium if hypocalcemia
- Noradrenaline is usual first line agent (e.g. supported by SSC guidelines)
- Alpha >> beta effects
- Increased SVR -> increased DBP & MAP, drives perfusion
- Increased venous tone -> preload
- If possible, avoid:
- pure alpha agonists (e.g. phenylephrine, midodrine, metaraminol)
- Worse outcomes in septic shock
- Less “ventriculo-arterial matching”
- Acceptable if low dose, likely short-term, and cause is pure vasodilation (e.g. peri-operative)
- Epinephrine
- Increased lactate and heart rate
- Acceptable alternative in low resource settings or inotropic effect required
- Dopamine
- Increased dysrhythmias
- pure alpha agonists (e.g. phenylephrine, midodrine, metaraminol)
- Alpha >> beta effects
- Second line agents are vasopressin and hydrocortisone
- Useful if:
- Apparent catecholamine resistance
- Avoid side effects of high dose single agent (e.g. catecholamines)
- Vasopressin
- Early use may be beneficial in some settings (e.g. VANCS trial for cardiac surgery; if coexistent pulmonary hypertension as has less pulmonary vascular constriction) but unclear evidence in septic shock
- Hydrocortisone
- Likely decreases NO/ NOS in VSM
- ADRENAL study showed decreased vasopressor duration in septic shock
- Useful if:
- Refractory vasoplegia
- Exclude/ treat other causes of shock
- Consider “NO antagonists” (improve vasoplegia but evidence is lacking for improved outcomes)
- Methylene blue (CI: serotonin syndrome, G6PD deficiency)
- Hydroxcobalamin
- Future/ experimental agents include:
- Angiotensin (ATHOS3 trial)
- Ascorbic acid
- Adrenomedullin
Q2.
Outline the specific therapies used in the management of:
a) phaeochromocytoma (25%)
b) myxoedema coma (25%)
c) hypercalcaemia (25%)
d) carcinoid syndrome (25%)
Learn more here:
Q3.
(a) List the thresholds for platelet transfusion in ICU patients (30%)
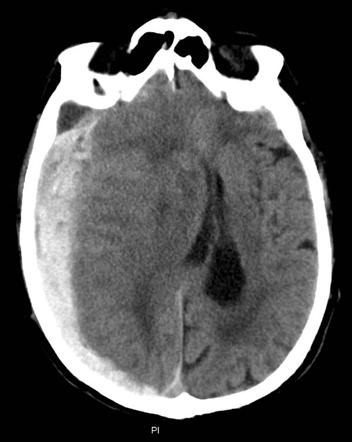
(b) Describe and interpret this non-contrast CT head image (20%)
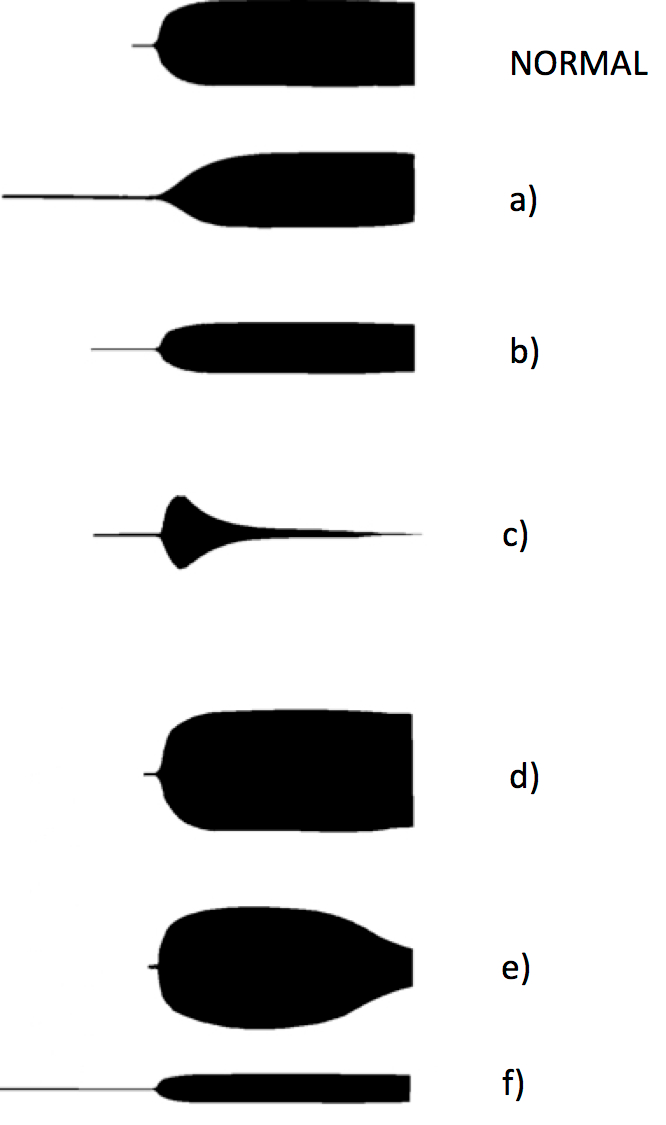
c) Suggest a cause of the hemostatic abnormailty, and appropriate therapy, for each of the TEG profiles a) to f) shown below: (50%)
Learn more here:
You can access all the previous practice questions since 2014 here:
https://docs.google.com/
See this link on INTENSIVE for exam resources:
//intensiveblog.com/