Labs and Lytes 009
Author: Anonymous
Reviewer: Chris Nickson
A 40 year-old man fell from a multi-story building. He sustained multiple traumatic injuries including a severe head injury. After 10 days in ICU he became increasingly tachypneic with a respiratory alkalosis, then was noted to have rhythmic right arm and facial jerking and developed a fixed, dilated right pupil. He was given treatment to lower his intra-cranial pressure, including hypertonic saline and a thiopentone infusion.
An urgent non-contrast CT head was performed; two axial slices are shown below:
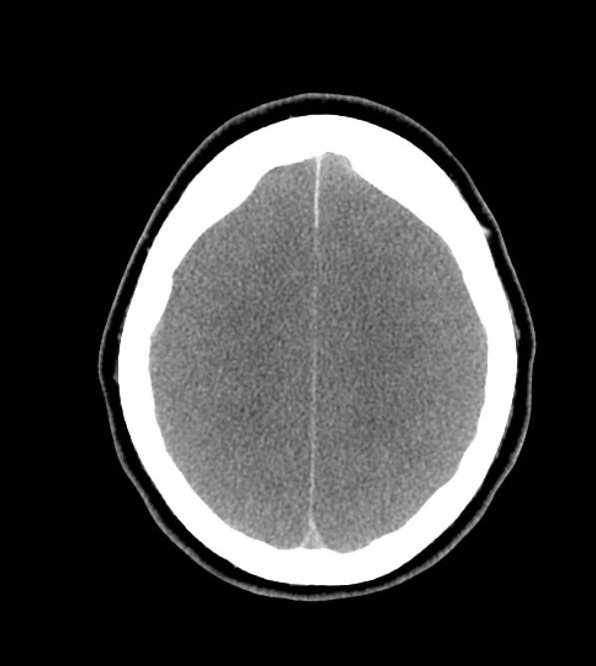
Image from Radiopaedia.org: http://goo.gl/PJYccG

Image from Radiopaedia.org: http://goo.gl/PJYccG
Q1. What are the CT head findings?
- Diffuse cerebral oedema, with loss of grey-white matter differentiation
- Complete effacement of sulcal spaces, and partial effacement of the ventricles
- Relative hyperdensity of the basal cisterns and sulci, HU 35-40, in keeping with pseudo subarachnoid haemorrhage
- Uncal herniation effacing the basal cisterns
Q2. What is pseudo-subarachnoid haemorrhage?
This is a CT head finding seen in patients with severe cerebral oedema characterised by relative hyperdensity of the basal cisterns and sulci
Theoretically due to:
- Displacement of low attenuated CSF by increased pressure
- Distension of the superficial vasculature
- Oedema of the adjacent cortex
Following the CT head the patient was reassessed and his progress was discussed with his family. A procedure was then performed.
During the procedure the patient’s monitor showed the following:
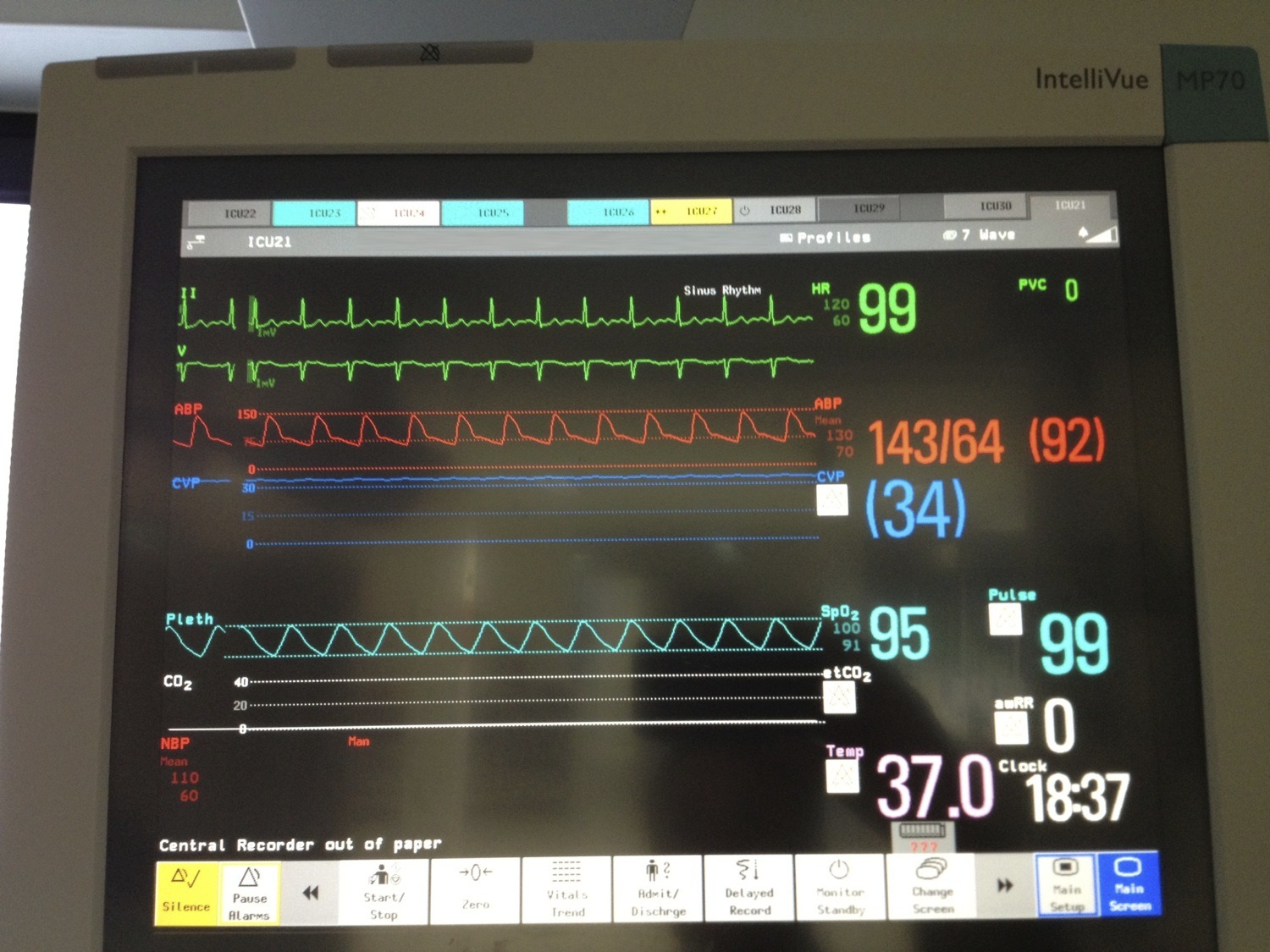
Click to enlarge
Q3. What procedure is being performed?
An apnoea test as part of clinical brain death testing, as indicated by the continuous ETCO2 reading of zero
Brain death testing involves demonstration of:
- absence of responsiveness
- absence of brainstem reflexes
- apnoea
There is also an incidental finding of elevated CVP with a flat trace, which may be artifactual.
Q4. What are the preconditions for this procedure?
Preconditions:
- cause for coma consistent with brain death
- at least 4 hours of observation during which other preconditions must be met (GCS 3, pupil non-reactive, no cough, apnoea)
- neuro-imaging consistent with acute brain pathology that could cause brain death
- normothermia (T>35C)
- normotension (SBP>90 or MAP>60mmHg in an adult)
- no sedation or analgesia (dependent on types of drugs used, renal and hepatic function; use antagonists if concerned)
- absence of severe electrolyte, metabolic and endocrine disturbances (glucose, Na+, PO43-, Mg2+, renal and hepatic function)
- no paralysis (use NMJ monitor or electromyography if concerned)
- ability to assess brain stem reflexes (at least one eye and ear)
- ability to perform apnoea test (doesn’t have severe hypoxic respiratory failure or have a high cervical spine injury)
Q5. How is the procedure performed?
Apnoea testing procedure
- Hyper-oxygenate for a period of 10min with 100% FiO2
- Ventilator is weaned (PEEP to 5, eucapnoea)
- Baseline ABG is taken
- If pt stable and SaO2>95% then patient can be disconnected from ventilator
- Oxygen is administered via a tracheal cannula (2L/min) or via CPAP (10cm H2O)
- Visual observation: 8-10min duration
- Repeat ABG prior to reconnection to the ventilator (expect rise of ~3 mmHg/min in PCO2 unless high O2 flow)
The test is deemed positive (consistent with brain death) if:
No respiratory response to:
- PaCO2 > 60mmHg (or an increase of 20mmHg)
- final arterial pH <7.3
References
- ANZICS Statement on Death and Organ Donation – 3.1 (2010)
- Radiopaedia.org — Diffuse axonal injury
- Radiopaedia.org — Pseudo-subarachnoid haemorrhage
- LITFL CCC — Brain Death
All case-based scenarios on INTENSIVE are fictional. They may include realistic non-identifiable clinical data and are derived from learning points taken from clinical practice. Clinical details are not those of any particular person; they are created to add educational value to the scenarios.