Everything ECMO 036
Author: Dr Gregory Brogan
Peer reviewers: Dr Sarah Yong, Dr Julia Coull
The development of Extracorporeal Membrane Oxygenation (ECMO) is intrinsically tied to our discoveries of the role of the circulatory system, oxygenation and the role of blood. As such, the scientific understanding which gave rise to ECMO came out of early organ perfusion experiments and extends through to the advances of the early 20th Century with the development of open-heart surgery and cardiopulmonary bypass (CPB) in the 1950s. Because of this, ECMO itself became a reality in the 1970s. Below you’ll find a timeline of a notable few of the scientists who contributed to these advances.
17th – 19th Century: The discovery of circulation
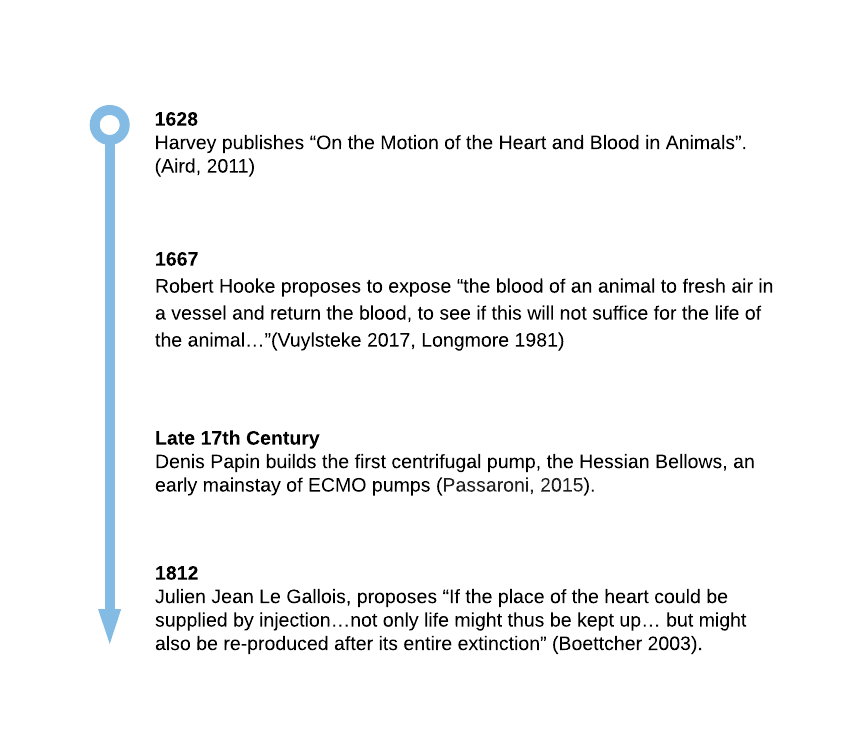
Centuries before the realisation of ECMO the basic concepts of circulation, extracorporeal oxygenation and artificial mechanical support were described by various scientists. Harvey’s publication of “On the Motion of the Heart and Blood in Animals”, which proposed the modern idea of the circulatory system overthrew 15 centuries of Galenic tradition (Aird, 2011). This set the scene for various scientists to develop early ideas about artificial oxygenation and mechanical circulatory support.
19th Century: From ideas to reality
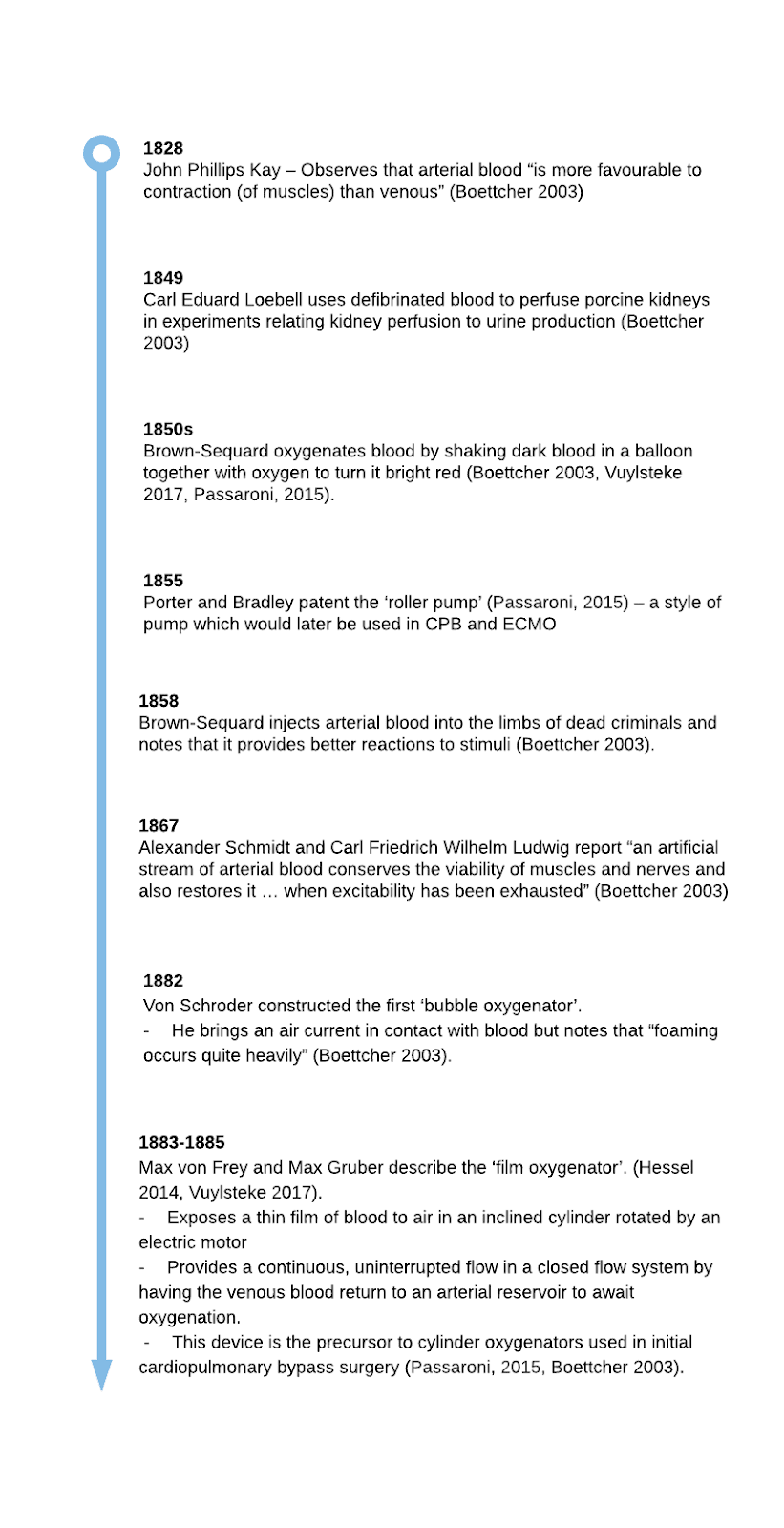
The 19th century saw various discoveries and experiments which demonstrated the role of oxygenated blood and organ perfusion. These experiments paved the way for the artificial perfusion of single organs in vitro and the proof of the concept that organ function can remain with artificially perfused organs. By the end of the 19th Century, von Frey and Gruber had developed a precursor to cardiopulmonary bypass – an artificial oxygenating machine which operated in a closed system.
Early 20th Century: The proof of concept
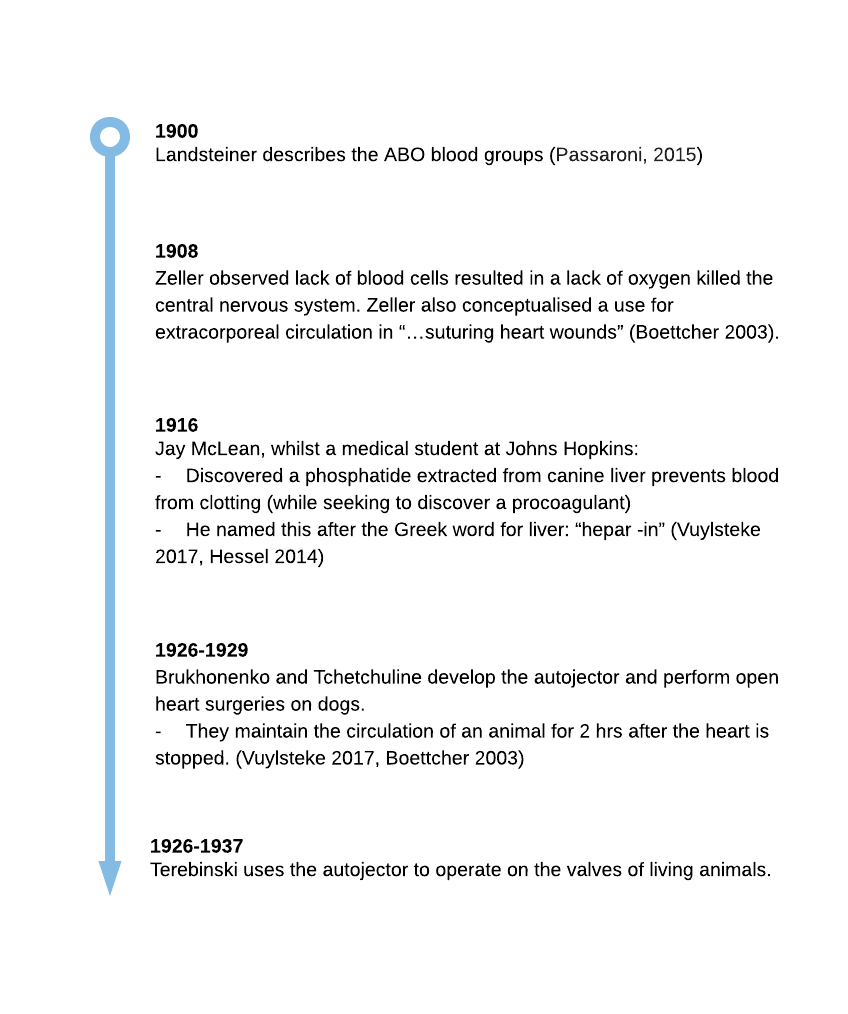
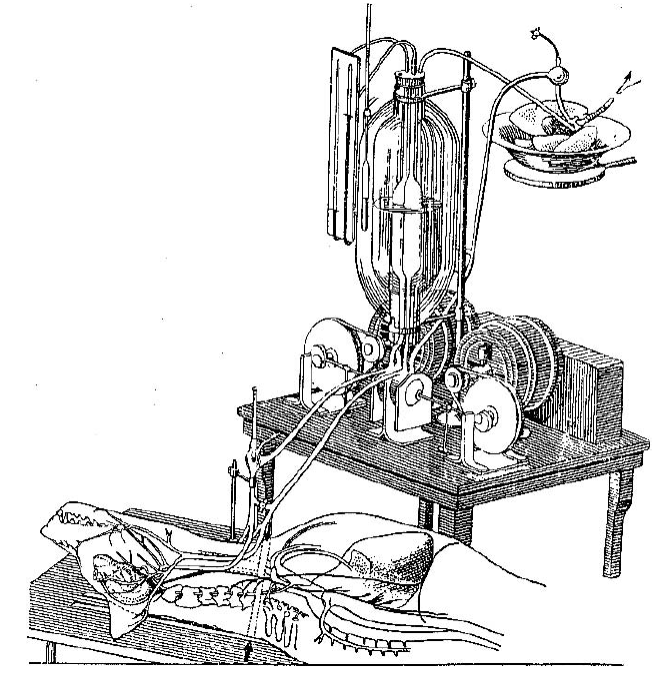
Until the 20th century the progress of ECMO was plagued by various practical issues, such as the bubbling and clotting of blood, which inhibited its use in humans. In fact, many earlier experiments defibrinated the blood thereby restricting it from use in living animals (Boettcher 2003). It wasn’t until discoveries in haematology allowed us to directly and safely use a patient’s own blood. By the 1920s, the technology for ECMO and cardiopulmonary bypass culminated in the invention of the ‘autojector’ by Brukhonenko and Tchetchuline. This device was used to perform whole body extracorporeal perfusion on a living dog. It consisted of 2 mechanical pumps with valves along with an oxygenator made of the ventilated lungs of a separate animal. One pump moved blood through the lungs and the second maintained systemic perfusion after the heart had stopped. (Boettcher 2003). This proof of concept provided sure footing to develop the first human ECMO machines.
1930s -1940s: The conception of ECMO in humans
The period of the 30s and 40s introduces us to John Gibbon Jr, the individual credited for the first successful use of cardiopulmonary bypass on a human. The catalyst for his work began after caring for a young woman with a massive pulmonary embolism (Hessel 2014). He conceived the idea of cardiopulmonary bypass to support her while performing an embolectomy. His and his wife’s early in vivo work helped to further establish the proof that an extracorporeal circulation could support a living organism and built the expertise required for the first clinical use of CPB. By the 1940s a few cardiac operations exist – they include the closure of patent ductus, a coarctation of the aorta repair, the Blalock-Taussig shunt procedure, a mitral commissurotomy and the closure of some atrial septal defects. Some of these are facilitated by deep hypothermia but in order to perform more complex open-heart operations it is evident that a system of Cardiopulmonary bypass is required (Stoney 2009).
1950s: The Introduction of Cardiopulmonary Bypass
This period marks the first actual use of cardiopulmonary bypass in human patients. Though Gibbon was the first to successfully use CPB, this new technique wouldn’t have flourished without the work of 2 important concurrent groups – one led by John Kirlkin at the Mayo Clinic and the other by C. Walton Lillehei at the University of Minnesota. By the end of this decade open heart surgery using cardiopulmonary bypass is a viable reality.
By the mid 1950s, oxygenators are mostly either film oxygenators or bubble oxygenators. The film oxygenators use a rotating cylinder, disc or screen to create a thin film of blood which is then exposed to oxygen. The bubbling oxygenator bubbles a stream of oxygen through a reservoir of blood in order to oxygenate it (Yeager 2017). These primitive oxygenators are plagued with issues of blood foaming which lead to trauma and the loss of products along with a high risk of arterial gas emboli. Thus, there is a push for new types of oxygenators. Other types of oxygenators used at this time include a monkey lung (by Mustard at Toronto medical school) (Stoney 2009) and an autologous lung (which pump through the patient’s own lungs) (Stoney 2009). Multiple groups, including Clowes and his team begin work on ‘membrane oxygenators’. They use sandwiched layers of a polymer membrane to physically separate the blood from a stream of pure oxygen and thus are the first clinical ‘membrane oxygenators’ (Vuylsteke 2017). Lots of different membranes were produced by many different groups but issues with consistent manufacturing complicate their wider introduction while the seepage of fluid (or ‘wetting’) and air emboli persist as issues (Yeager 2017).
1960s: The reality of Cardiopulmonary bypass
By the 1960s cardiopulmonary bypass was gaining momentum and open-heart surgery was viable. This decade would also lead to the development of artificial heart valves, the introduction of coronary artery bypass grafting and the first heart transplant (Hessel 2014). Symbolically, it was during the 1960s that the term “perfusionist” is coined by Bennett Mitchell. (As tempting as it would be to continue to discuss the history of cardiothoracic surgery, I’ll focus the rest of this to the development of ECMO out of Cardiopulmonary Bypass).
By the 1960s cardiac bypass was reliable enough to perform relatively quick open-heart surgeries. However, in order to support a patient for an extended duration as in ECMO, further modifications would have to be made. For instance, the development of silicone membranes for oxygenators through the 1960s prolonged the lifespan of circuits and allowed their ongoing use for weeks (Bartlett 2005).
1970s: The Birth of ECMO
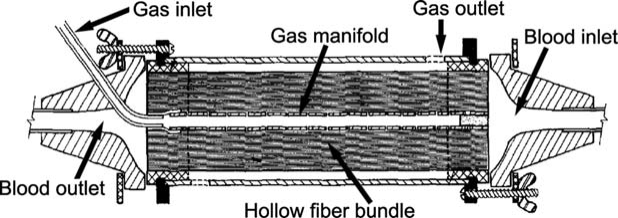
The success of the 1950s and 60s gave way to the advances in the 1970s. The 1970s saw the first use of cardiopulmonary bypass in a non-surgical patient – this can be said to be the birth of ECMO as we know it. Over this decade case reports build regarding the use of cardiopulmonary bypass in cardiac failure and respiratory failure of various causes (Bartlett 2005). Furthermore, this decade is important for various advances in oxygenators. Hollow fibre oxygenators are introduced (Yeager 2017). They are constructed similar to renal dialysers where small tubes are used to separate the blood and gas thereby providing a large surface to volume ratio. However, despite the initial successes of ECMO, the 1970s silicone membrane oxygenators are plagued with many coagulation issues. Microporous polypropylene hollow fibre oxygenators are developed which reduce many of these coagulation issues and further improve gas transport (Yeager 2017). Despite this advancement new issues like ‘wetting’ arise. This is where plasma would be driven through the micropores in the membrane by the pressure of the blood causing soapy bubbles to form and limiting the lifespan of the membrane (Yeager 2017).
Membrane oxygenators then are later tweaked to become ‘cross flow’ hollow fibre oxygenators – where blood flows outside the cross woven hollow fibres instead of within while the fibres contain the flowing oxygen. Despite the technological advancements, early studies fail to show a benefit of ECMO and thus it suffers a significant setback in its widespread adoption (Cavarocchi 2017). This speed bump causes many to stop offering it (Vuylsteke 2017). However, the experience in paediatrics and neonatology would be very different and it would prove to be an important, life-saving treatment (Wolfson 2003). Compared to the current technology, the 1970s technology was still relatively archaic though later this decade, centrifugal pumps begin to be used (Passaroni, 2015). These pumps consist of a central rotating impeller that spins and generates centrifugal force to pump blood forward. As an aside, this decade also saw the introduction of the ballooned tipped pulmonary artery catheter introduced by Swan and Ganz.

1980s-1990s: ECMO in wider distribution
The period of the 1980s-1990s saw further development in the hardware of ECMO along with its wider distribution. During this time, the hollow fibre oxygenators with extraluminal crossflow of blood became commonplace (Yeager 2017). Cyclosporine was introduced as an antirejection medication which vastly improved the survival rates of heart transplantation. This made it a more viable treatment option for end stage heart failure (Hessel 2014). Furthermore, ventricular assist devices also take off as therapy for end stage heart failure.
1990-2000s: ECMO as we know it
By the late 20th century ECMO had become a viable treatment, especially in paediatrics and neonatology where “every major childrens’ hospital” had a team or plan to triage ECMO cases (Bartlett 2005). Further important advances in circuits take place over this time – Earlier ECMO circuits had silicone membranes and used roller pumps. These circuits were complicated by wetting. The average ECMO run would require perhaps 2-3 oxygenators. This decade saw the introduction of Polymethylpentene (PMP) oxygenators and the further spread of centrifugal pumps. PMP oxygenators reduced the “wetting” issue of previous membranes. PMP hollow fibre oxygenators now become the standard of care (Yeager 2017). Centrifugal pumps are introduced over the previously used roller pumps. This new ECMO now boasts reduced haemolysis, heparin use, transfusion requirements and less complications (Cavarocchi 2017).
2000s – 2010s: Modern ECMO in Clinical Trials
By the mid 2000s, ELSO data reveals that ECMO is primarily used for congenital and paediatric diseases. ELSO begins creating guidelines for training, staffing and equipment (Cavarocchi 2017). The use of ECMO in refractory respiratory failure in adults continues and in 2009 the H1N1 influenza epidemic strikes. ECMO is used in refractory respiratory failure with clinical success, with some publications from the time showing a 71% survival in patients failing conventional therapy for ARDS (ANZ ECMO 2009). The CESAR trial is published. It is a large multicentre randomised controlled trial in the United Kingdom featuring an Intention to treat analysis of conventional ventilation vs transfer to an ECMO referral centre. It showed a benefit with transfer to ECMO centre and a mortality rate of 37 vs 53%. However, there are many criticisms of this publication and interpetation of the study is frustrated by the fact that many patients who were transferred to the ECMO centre were not put on ECMO. (Peek 2009)
2010-2021: Modern ECMO Established
By this time, the modern ECMO machine utilises centrifugal pumps and PMP membranes. Some models now combine the pump and oxygenator together. Though there is still variation in how it is used and implemented between centres (Cavarocchi 2017) the role for ECMO remains a bridge to recovery or transplant as it is not curative in itself (Yeager 2017). In 2018 the EOLIA Trial is published. It is stopped early and demonstrates no benefit at day 60 in terms of mortality when compared with conventional mechanical ventilation, though again, interpretation is confounded as ECMO was used to rescue the control arm (Combes 2018). In 2020 the COVID-19 pandemic strikes leading to a huge burden of cases of respiratory failure. ECMO becomes an important treatment during this time and we await to see its utility.
References
- Aird WC. Discovery of the cardiovascular system: from Galen to William Harvey. J Thromb Haemost. 2011 Jul;9 Suppl 1:118-29. doi: 10.1111/j.1538-7836.2011.04312.x. PMID: 21781247.
- Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators, Davies A, Jones D, Bailey M, Beca J, Bellomo R, Blackwell N, Forrest P, Gattas D, Granger E, Herkes R, Jackson A, McGuinness S, Nair P, Pellegrino V, Pettilä V, Plunkett B, Pye R, Torzillo P, Webb S, Wilson M, Ziegenfuss M. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA. 2009 Nov 4;302(17):1888-95. doi: 10.1001/jama.2009.1535. Epub 2009 Oct 12. PMID: 19822628.
- Bartlett RH. Esperanza: The First Neonatal ECMO Patient. ASAIO J. 2017 Nov/Dec;63(6):832-843. doi: 10.1097/MAT.0000000000000697. PMID: 29084039.
- Bartlett RH. Extracorporeal life support: history and new directions. ASAIO J. 2005 Sep-Oct;51(5):487-9. doi: 10.1097/01.mat.0000179141.08834.cb. PMID: 16322701.
- Boettcher, W., Merkle, F. (2003). History of Extracorporeal Circulation: The conceptional and developmental period. The Journal of Extra-corporeal Technology. 35 (3): 172-0183.
- Cavarocchi NC. Introduction to Extracorporeal Membrane Oxygenation. Crit Care Clin. 2017 Oct;33(4):763-766. doi: 10.1016/j.ccc.2017.06.001. PMID: 28887925.
- Combes A, Hajage D, Capellier G, Demoule A, Lavoué S, Guervilly C, Da Silva D, Zafrani L, Tirot P, Veber B, Maury E, Levy B, Cohen Y, Richard C, Kalfon P, Bouadma L, Mehdaoui H, Beduneau G, Lebreton G, Brochard L, Ferguson ND, Fan E, Slutsky AS, Brodie D, Mercat A; EOLIA Trial Group, REVA, and ECMONet. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018 May 24;378(21):1965-1975. doi: 10.1056/NEJMoa1800385. PMID: 29791822.
- Extracorporeal Life Support Organization (2021). ELSO Homepage. https://www.elso.org/TrainingCourses.aspx. Last Accessed (1/3/21)
- Hessel EA 2nd. A Brief History of Cardiopulmonary Bypass. Semin Cardiothorac Vasc Anesth. 2014 Jun;18(2):87-100. doi: 10.1177/1089253214530045. Epub 2014 Apr 10. PMID: 24728884.
- Longmore, D.B. (ed.)Wyatt, R. (1981) Towards Safer Cardiac Surgery: Chapter 29 Long Term Extracorporeal Membrane Oxygenation. MTP Press 1981. Page 475
- Passaroni AC, Silva MA, Yoshida WB. Cardiopulmonary bypass: development of John Gibbon’s heart-lung machine. Rev Bras Cir Cardiovasc. 2015 Mar-Apr;30(2):235-45. doi: 10.5935/1678-9741.20150021. PMID: 26107456; PMCID: PMC4462970.
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D; CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009 Oct 17;374(9698):1351-63. doi: 10.1016/S0140-6736(09)61069-2. Epub 2009 Sep 15. Erratum in: Lancet. 2009 Oct 17;374(9698):1330. PMID: 19762075.
- Stoney WS. Evolution of cardiopulmonary bypass. Circulation. 2009 Jun 2;119(21):2844-53. doi: 10.1161/CIRCULATIONAHA.108.830174. PMID: 19487602.
- Vuylsteke, A. et al (2017) ECMO in the Adult Patient: Chapter 1 A Brief History of ECMO. Cambridge University Press 2017. Pages 1-8.
- Wolfson PJ. The development and use of extracorporeal membrane oxygenation in neonates. Ann Thorac Surg. 2003 Dec;76(6):S2224-9. doi: 10.1016/j.athoracsur.2003.09.003. PMID: 14667691.
- Yeager T, Roy S. Evolution of Gas Permeable Membranes for Extracorporeal Membrane Oxygenation. Artif Organs. 2017 Aug;41(8):700-709. doi: 10.1111/aor.12835. Epub 2017 Jan 19. PMID: 28105685.
Hello, my name is bree, in 1997, I was the successful 19year old female to be transported on ECMO from maroondah hospital to st Vincent’s hospital in Melbourne.ECMO with Dr Alex Rosellian ,Simon ,Jeoff , an the profusionist team saved my life, for that, I am eternally grateful xxxx
Wow, hope you are doing well Bree!
Hi Intensiveblog Team,
What a delight of a summary of the evolution of ECMO. I appreciate diving far further than Gibbon and the 1930′ in preparing a presentation on the history of ECMO.
On a side note, I would bring your attention to the timeline where Bartlett and baby Esperanza are mentioned twice (under 1974 and 1976). It is one case, originally published in 1976 in a case series of 4, by Bartlett. Hope this was helpful.
Excellent summary