Labs and Lytes 028
Authors: Malachy Feeney, David Humphreys, Bianca Macula and Virginia Newcombe
Peer Reviewers: Chris Nickson, David Anderson
Brian Cushing is an 18-year-old male admitted to your ICU post a high sped MVA from which he sustained a severe traumatic brain injury and pelvis fracture. He had a pre-intubation GCS of 8 and evidence of DAI on his CT head. Prior to arriving at the unit he was taken to theatre where an EVD was inserted.
Q1. What is an EVD?
An Extraventricular Drain or External Ventricular Drain (EVD), is one of the most common and most important life-saving procedures in the setting of acquired brain injury. It is commonly used for subarachnoid haemorrhage, traumatic brain injury and other conditions associated with acute hydrocephalus.
EVDs are closed sterile systems that allow monitoring and treatment of raised intra-cranial pressure (ICP). They consist of intraventricular catheters typically placed directly into the anterior horn of the lateral ventricle through a burr hole in the skull, attached to a pressure transducer and an external drainage and monitoring system. They are considered to be the gold standard for measuring ICP.
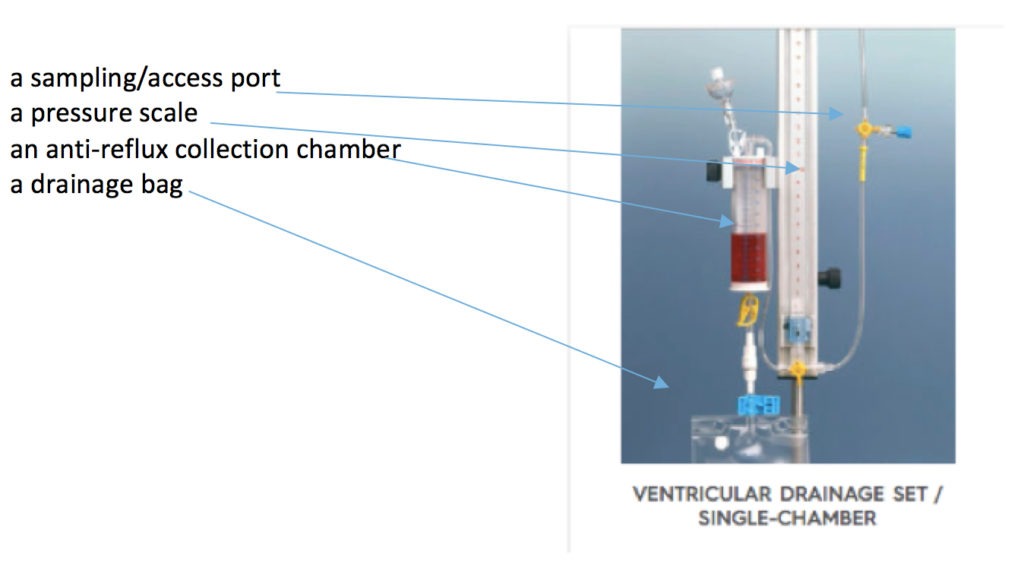
Q2. What are the components of an EVD?
Insertion of an EVD prevents intracranial hypertension by diverting cerebrospinal fluid (CSF) and intraventricular blood from the lateral ventricles to an external reservoir. It may also allow continuous intracranial pressure monitoring to help guide brain targeted resuscitation in these critically ill patients.
The ventricular catheter and external drainage system has several components:
The bedside nurse asks you how to set up the EVD as she cannot read the neurosurgical registrar’s operative note has gone missing. Unfortunately, he is not currently available as he is scrubbed in theatre.
Q3. Where is it recommended that the arterial transducer is placed if a patient has an EVD placed for ICP management?
The current Brain Trauma Foundation guidelines focus on targeted management of ICP and CPP where:
CPP = MAP –ICP
Most guidelines currently recommend that the arterial transducer is set at approximately the level of the foramen of Monro which is considered to be approximately the level of the external auditory meatus or the level of the tragus rather than the phlebostatic axis (heart level) to enable more accurate calculation of CPP. The transducer position should be change to remain at the level of the tragus regardless of patient position. Individual differences in cerebral arterial and venous circulations mean that it not possible to determine a coefficient (C) that accurately takes this into account if the transducer is left at the phlebostatic axis.
MAP brain = MAP heart – (water column between the heart and brain x C)

Image from: http://www.slideshare.net/drtirumal/raised-icp (click image for source)
Q4. How is the height of the EVD decided?
The level of the ventricles is estimated to provide the zero point. The difference in height between the ventricles and the collection system chamber creates both a pressure gradient and a safety valve. The height of the drip chamber equates to the pressure inside of the head or intracranial pressure (ICP). This pressure must be reached before any CSF will drain into the collection system. Accurate placement and zeroing of the system is important. For example, if the transducer is above Foramen of Monro, falsely low ICP and insufficient drainage of CSF may occur, and intracranial hypertension would go undetected.
For a patient with SAH and an unsecured aneurysm it is important to set the initial height of the EVD “high” so that CSF is not drained too quickly to avoid a rapid change in transmural pressure across the aneurysm wall which may lead to re-bleeding.
At The Alfred the standard EVD starting drain height tends to be +5 mmHg for TBI patients and +10 to 15 mmHg for SAH.
It is important to note that when the EVD is draining (“venting”) CSF the ICP measurements are not measured.
You are advised the next morning on handover that Brian has spiked a fever overnight.
Q5. What are you concerned about, and what are your next steps?
EVD-related ventriculitis is unfortunately not an uncommon occurrence in patients with EVDs in situ. Rates range from <1% to 40% (10-20% in most studies), with a mortality rate of 10-75%.
The current proposed mechanisms of EVD-related infection are:
- inoculation of skin flora during insertion, and/or
- contamination and colonization of the components during the post-operative period, with subsequent retrograde infections appearing when patients are brought to the wards.
EVD-related infections include: ventriculitis, meningitis, cerebritis, brain abscess and subdural empyema.
If a patient is febrile, or there is an unexplained decrease in GCS score, a visible change in CSF, or an elevation in systemic WCC, then a CSF sample should be aspirated and cultured. Clinical features such headache, nausea and emesis, fever, focal neurological deficits, and raised ICP may be subtle in EVD-related infections – no single parameter can predict OR exclude ventriculitis.
CSF analysis suggestive of ventriculitis include:
- high WCC
- high/normal protein
- cell index (leucocytes:erythrocytes in CSF divided by leucocytes:erythrocytes in blood) is usually 1 in healthy patient and increases in up to 5+ in ventriculitis. The cell index falls with antibiotic use.
The causative organisms are typically S.aureus, coagulase-negative S.epidermis, gram-negative bacteria. Consider fungi in the immunocompromised patient population.
While other Health networks may recommend daily CSF sampling, Alfred Health do not recommend routine CSF cultures in a patient that is not febrile in the first week of insertion. After 5 days the risk of infection increases progressively, if a catheter has been in >1week, it is not unreasonable to send occasional cultures (Monday, Wednesday, Friday) even if the patient is afebrile.
Antibiotics may be given systemically (e.g. vancomycin and ceftazidime), or intrathecally via the EVD, depending on local protocols. If ventriculitis occurs then the EVD should be removed as soon as it is safe to do so.
The nurse calls to let you know the EVD has stopped draining.
Q6. What could have caused this and what can you do?
EVDs may block due to a variety of reasons:
- a blockage in the system; by clots or debris
- accidentally clamped EVD
- dislodgement from within the ventricles
- CSF leak or rising pressure
If CSF output is less than documented reportable limits, the EVD is not oscillating, or the ICP waveform is flat, it may lead inadequate drainage of CSF which can lead to an increased ICP. Ensure the Neurosurgeons are notified, and the patient is examined and monitored for signs of increased ICP.
If a catheter appears to be blocked:
- exclude damage to the EVD system
- lower drain and observe for CSF movement
- consider changing the EVD drainage set
- consider aspiration and/or flushing of the catheter using an aseptic technique
It is now Day 8 and Brian’s ICPs have been < 20mmHg for 48 hours with little intervention needed and minimal drainage of CSF.
Q7. When should an EVD be removed?
Duration of EVD placement will depend upon both:
- (the clinical indication for insertion, and
- ongoing ICP stability
In the setting of stable ICP measurements, a typical removal strategy is to gradually raise the level of the EVD over several days, followed by clamping (a “clamp trial”).
In patients with persisting elevated ICP readings (requiring active medical management +/- CSF venting) or worsening neurology/hydrocephalus while the EVD is clamped, consideration will be given to placement of a ventriculoperitoneal (VP) shunt. Numerous studies have attempted to assess predictors for eventual shunt requirement: findings are variable and predilection for development of chronic hydrocephalus is likely multifactorial.
Given the risk posed by infection (ventriculitis), regular (daily) assessment should be made regarding any persisting EVD requirement and whether the drain can be removed.
References and links
- Alfred ICU Guidelines:Intracranial Pressure (ICP) Monitoring and Extraventricular Drains (EVD). 2006 [cited 6 June 2016]. Available from: http://www.alfredicu.org.au/assets/Documents/Services-Docs/Trauma-Docs/ICP-and-EVD-Guideline.pdf
- Clinical Guidelines: External Ventricular Drains and Intracranial Pressure Monitoring. Rch.org.au. 2016 [cited 6 June 2016]. Available from: http://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/External_Ventricular_Drains_and_Intracranial_Pressure_Monitoring/#EVD
- Joint position statement by the Councils of the Neuroanaesthesia Society of Great Britain and Ireland (NASGBI) and the Society of British Neurological Surgeons (SBNS) with regards to the calculation of cerebral perfusion pressure in the management of traumatic brain injury. 2014 [cited 6 June 2016]. Available from: http://naccsgbi.org/wp-content/uploads/2015/03/Final_Revised_Joint_CPP_statement_Aug_2014.pdf
- Nickson CP. External Ventricular Drain. Lifeinthefastlane.com. 2016 [cited 6 June 2016]. Available from: http://lifeinthefastlane.com/ccc/external-ventricular-drain/
- Nickson CP. Ventriculitis. Lifeinthefastlane.com. 2016 [cited 6 June 2016]. Available from: http://lifeinthefastlane.com/ccc/ventriculitis/
- Sang ACO, Leung GKK. External Ventricular Drain Infections. In: Pant S, Cherin I. Hydrocephalus. InTech; 2012. [open access book]
All case-based scenarios on INTENSIVE are fictional. They may include realistic non-identifiable clinical data and are derived from learning points taken from clinical practice. Clinical details are not those of any particular person; they are created to add educational value to the scenarios.
Pingback: Global Intensive Care | Own the EVD!