Labs and Lytes 033
Author: David Humphreys
Reviewer: Sarah Yong, Chris Nickson
A 59-year-old female patient has had a prolonged stay in your ICU.
This her most recent chest radiograph:
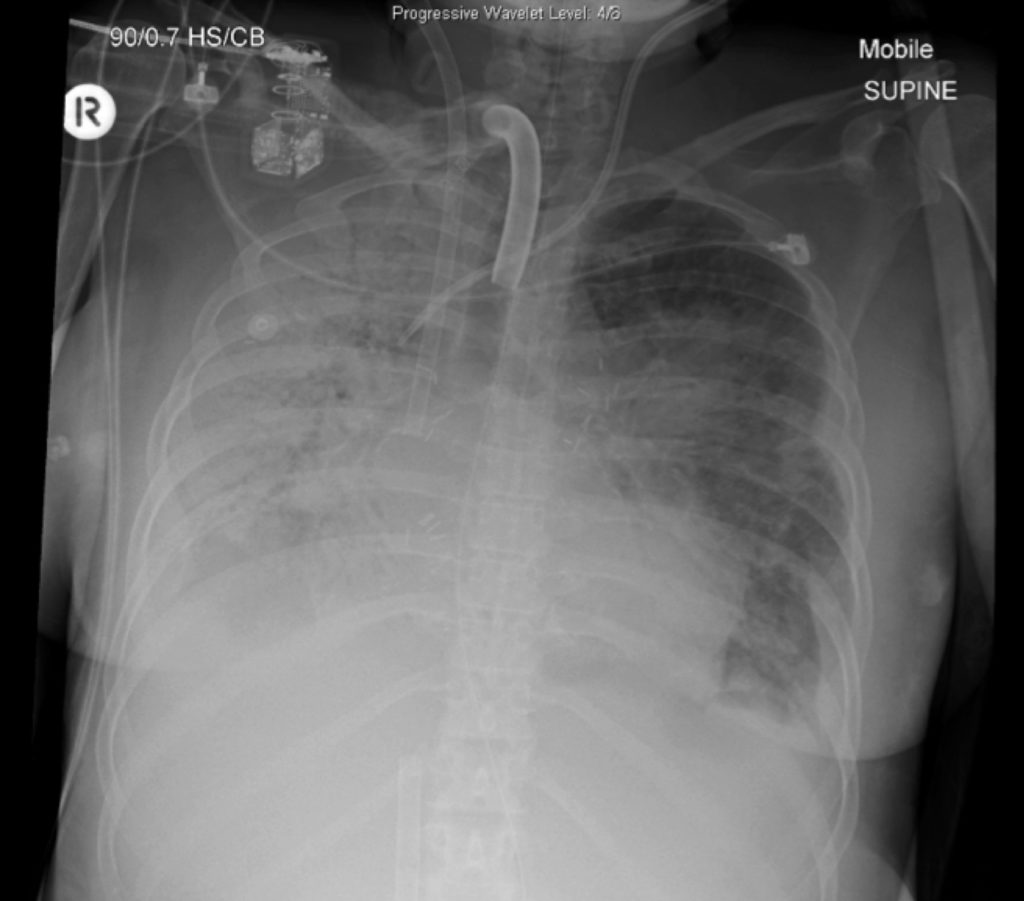
Figure 1. Chest radiograph
Q1. Describe and interpret the chest radiograph.
This is a supine mobile CXR with extensive pathology and numerous hardware in situ.
- The most striking abnormality is complete opacification of the right lung field, consistent with diffuse consolidation
- Airspace opacities also involve the left lower and upper lobes
- VV ECMO cannulae appropriately placed in the right internal jugular vein (IJV) (tip at junction between superior vena cava (SVC) and right atrium (RA)) and right femoral vein (RFV) (tip is in inferior vena cava (IVC))
- Tracheostomy tube, left internal jugular central venous line, mediastinal surgical clips, and a nasogastric tube are also visible
The presence of extensive pulmonary pathology, tracheostomy and VV ECMO cannulae indicate a patient with severe pulmonary disease and critically impaired gas exchange. The number of small metallic vascular clips in the centre of the image (posterior to the mediastinal shadow) are the result of a recent bilateral sequential lung transplant for idiopathic pulmonary hypertension.
In an immune-suppressed transplant patient, the possible causes of the consolidation are numerous. Fungal infection is an important possibility.
References
- Nickson CP. Lung transplant. Critical Care Compendium, Lifeinthefastlane.com. [Accessed 3 November 2017]. Available at URL: https://lifeinthefastlane.com/ccc/lung-transplant/
- Nickson CP. Transplant patients in ICU SDL. INTENSIVEblog.com 18 August 2017 [Accessed 3 November 2017]. Available at URL: https://intensiveblog.com/resources/transplant-patients-icu-sdl/
- Pilcher D. Lung Transplantation. INTENSIVEblog.com 30 July 2017. [Accessed 3 November 2017]. Available at URL: https://intensiveblog.com/lung-transplantation-david-pilcher/
All case-based scenarios on INTENSIVE are fictional. They may include realistic non-identifiable clinical data and are derived from learning points taken from clinical practice. Clinical details are not those of any particular person; they are created to add educational value to the scenarios.